At a glance
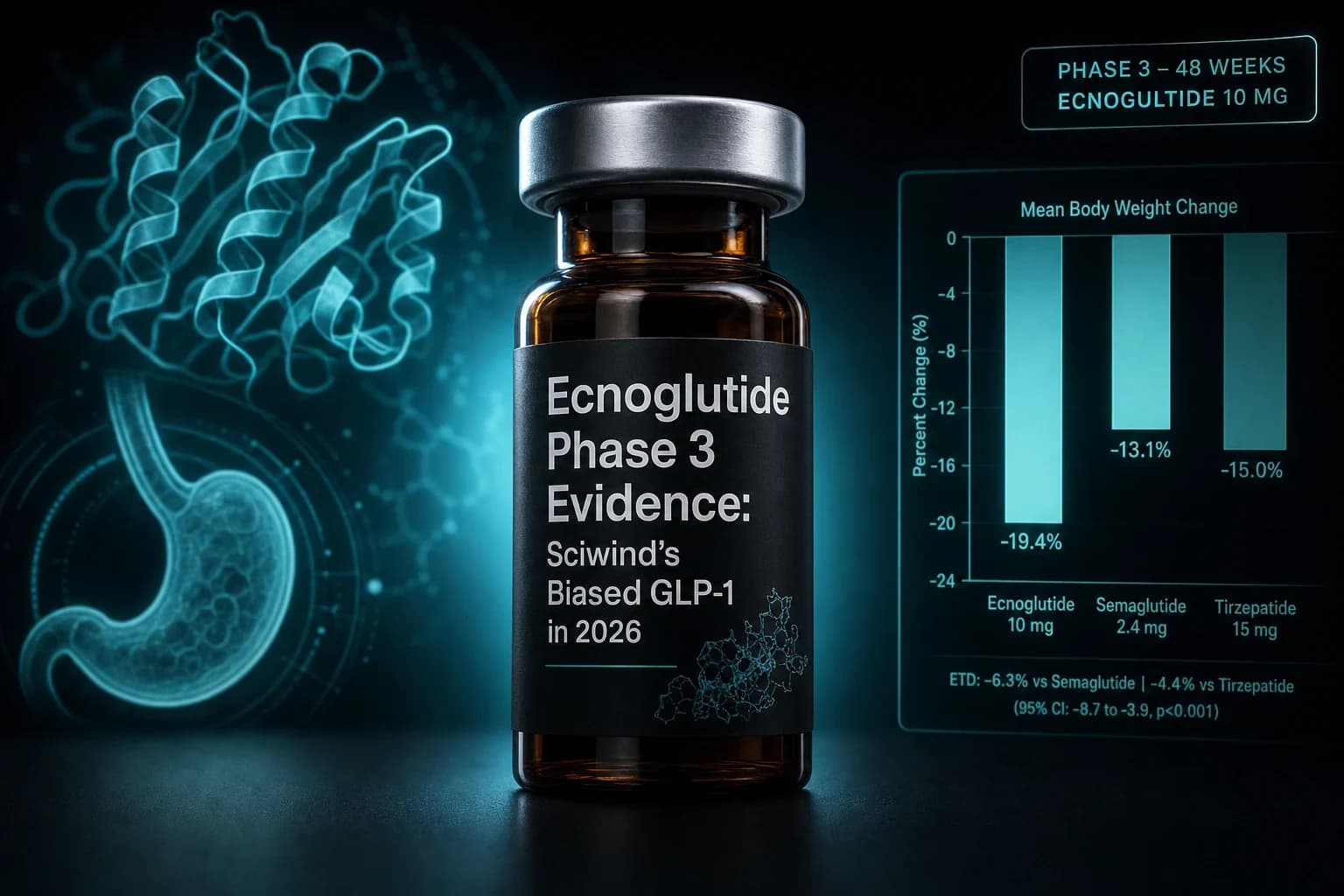
- Ecnoglutide (XW003) is the first cAMP signaling-biased GLP-1 receptor agonist to reach Phase 3, engineered to activate cAMP with reduced beta-arrestin recruitment.
- SLIMMER Phase 3 in Chinese adults with overweight or obesity (Ji et al. Lancet Diabetes Endocrinol 2025, PMID 40555243): placebo-adjusted weight change of -9.6%, -13.0%, and -15.1% at 48 weeks for the 1.2, 1.8, and 2.4 mg once-weekly doses.
- EECOH-1 Phase 3 in Chinese T2D monotherapy (Nature Communications 2026, DOI 10.1038/s41467-025-68165-7): HbA1c reduction of 2.43 percentage points from baseline in the 1.2 mg group vs placebo at week 24.
- EECOH-2 Phase 3 vs dulaglutide (He et al. Lancet Diabetes Endocrinol 2025, PMID 40854315): non-inferior HbA1c reduction at 52 weeks with greater weight loss than dulaglutide 1.5 mg.
- China NMPA approved ecnoglutide injection for chronic weight management in September 2025; no US, EU, or UK approval as of July 2026.
- A 20-week interim of the head-to-head SLIMMER-UP-SWITCH Phase 2 (ADA 2026 late-breaker) reported -12.8% weight change on ecnoglutide 2.4 mg vs -9.5% on semaglutide 2.4 mg. Interim, open-label, not yet peer-reviewed.
China quietly approved the first cAMP-biased GLP-1 in 2025. The Phase 3 numbers are worth reading in full.
Ecnoglutide (XW003) is a weekly subcutaneous GLP-1 receptor agonist developed by Hangzhou Sciwind Biosciences. It is the first GLP-1 analog engineered specifically to activate cAMP downstream of the GLP-1 receptor while dialing back beta-arrestin recruitment. That receptor bias is the core mechanistic idea, and it is the reason a Chinese biotech was able to publish a Phase 3 obesity trial in The Lancet Diabetes & Endocrinology in June 2025 that landed a placebo-adjusted 15.1% body weight reduction at 48 weeks.
If your mental model of the GLP-1 field ends at semaglutide, tirzepatide, and orforglipron, ecnoglutide fills in an important gap. It is not a triple agonist. It is not oral. It is a single-target GLP-1 monoagonist tuned at the receptor level, and its Phase 3 data now cover both obesity (SLIMMER) and Type 2 diabetes (EECOH-1, EECOH-2). It also has an interim head-to-head against semaglutide 2.4 mg that reads well, presented as a late-breaker at ADA 2026.
The catch is that everything to date is a Chinese-population study, the regulatory approval is China only, and the head-to-head is 20 weeks in and open-label. This walkthrough covers what the peer-reviewed data actually show, how the biased-agonism mechanism connects to the efficacy signal, and where ecnoglutide sits against the orforglipron oral GLP-1 evidence and the broader Chinese GLP-1 pipeline (see also the mazdutide GLP-1/glucagon dual agonist read).
What "cAMP-biased" means at the receptor
The GLP-1 receptor is a class B G protein-coupled receptor. When a ligand binds, two things happen at different speeds. The receptor couples to Gs and drives adenylyl cyclase, raising intracellular cAMP. Almost immediately, beta-arrestin 1 and 2 are recruited to the phosphorylated tail of the receptor, triggering desensitization, internalization, and downstream MAPK signaling. Native GLP-1 does both. So do semaglutide, liraglutide, and dulaglutide. That balance shapes both efficacy and tolerability.
Biased agonism means designing a ligand that pushes one arm harder than the other. Ecnoglutide is engineered to activate the cAMP arm while recruiting beta-arrestin less strongly than a full agonist would. The theoretical case, developed for other class B receptors before it was applied here, is that reduced beta-arrestin recruitment slows receptor desensitization, prolongs pancreatic beta-cell signaling per dose, and may reduce some tolerability liabilities that track with arrestin-driven pathways.
Whether that translates into a meaningful clinical benefit is exactly what the SLIMMER and EECOH trials were designed to test. The relevant background papers here are the receptor pharmacology work from Jones and colleagues on GLP-1 receptor bias in beta cells (Jones et al., Nat Commun 2018, PMID 30310072) and the earlier Zhang lab structural work on class B GPCR conformational states. Ecnoglutide is not the first molecule to try this. It is the first to get through a positive Phase 3 with the biased-agonist rationale intact.
Route of administration is standard: a once-weekly subcutaneous injection with abdominal, thigh, or upper-arm sites. Half-life supports steady weekly dosing. The Phase 3 dose ladder in obesity used 1.2 mg, 1.8 mg, and 2.4 mg once weekly with a graded titration from a 0.3 mg starting dose over 16 weeks.
Note: "Biased" does not mean "safer" or "better" as a general rule. It means the ligand shifts the balance between two signaling arms. Whether that shift is clinically valuable depends on the disease and the endpoint. For ecnoglutide, the case has to rest on trial data, not mechanism narrative.
SLIMMER Phase 3: 15.1% placebo-adjusted weight loss at 48 weeks
The SLIMMER trial is the pivotal obesity dataset. It was a multicenter, randomized, double-blind, placebo-controlled Phase 3 study run across 36 sites in China, published by Ji and colleagues in The Lancet Diabetes & Endocrinology in 2025 (PMID 40555243).
Eligible participants were adults aged 18 to 75 with a BMI of 28 kg/m² or higher, or 24 kg/m² or higher with at least one weight-related comorbidity, and without Type 1 or Type 2 diabetes. Randomization was to subcutaneous ecnoglutide at 1.2 mg, 1.8 mg, or 2.4 mg once weekly, or matched placebo, for 48 weeks, followed by an off-drug extension. Titration ran over the first 16 weeks. The primary endpoint was the percentage change in body weight from baseline to week 48.
| Endpoint (week 48) | Placebo | Ecnoglutide 1.2 mg | Ecnoglutide 1.8 mg | Ecnoglutide 2.4 mg |
|---|---|---|---|---|
| Mean weight change | approximately -1.5% | -11.1% | -14.5% | -16.6% |
| Placebo-adjusted change | ref | -9.6% | -13.0% | -15.1% |
| Achieved 5% or greater loss | 21% | 77% | 84% | 87% |
| Achieved 10% or greater loss | 8% | 55% | 68% | 74% |
| Achieved 15% or greater loss | 3% | 33% | 45% | 55% |
Two features of this readout matter. First, the dose-response is clean and monotonic across three active arms, which is what you want to see if the mechanism story holds. Second, the 2.4 mg placebo-adjusted 15.1% at 48 weeks sits in the same weight-loss range as semaglutide 2.4 mg in the STEP-1 obesity trial (Wilding et al., NEJM 2021, PMID 33567185), which reported a placebo-adjusted 12.4% at 68 weeks in a mostly non-Chinese population. Different trial durations, different populations, and different baseline BMIs make a direct number-to-number comparison invalid. But it puts ecnoglutide in the mono-agonist top tier rather than the middle of the pack.
The trial also captured cardiometabolic parameters. Ecnoglutide dose-dependently reduced waist circumference, systolic blood pressure, LDL cholesterol, triglycerides, HbA1c, fasting glucose, and high-sensitivity CRP versus placebo. Whether those secondary reductions translate into cardiovascular event reduction is the question that a dedicated cardiovascular outcomes trial would have to answer, and none is currently reported for ecnoglutide.
Bottom line: SLIMMER is the strongest single trial in the ecnoglutide file. A 15.1% placebo-adjusted weight change at 48 weeks in a Phase 3 monoagonist is a genuinely notable result, and it justifies serious attention to the biased-agonism thesis. It does not, on its own, prove ecnoglutide beats semaglutide in the same population.
EECOH-1 Phase 3: T2D monotherapy at 24 weeks
The Type 2 diabetes evidence anchors on EECOH-1, a multicenter, randomized, double-blind, placebo-controlled Phase 3 trial run at 32 sites in China. Results were published in Nature Communications in January 2026 (DOI 10.1038/s41467-025-68165-7). The trial enrolled 211 Chinese adults with Type 2 diabetes inadequately controlled by diet and exercise alone, and randomized them 1:1:1 to ecnoglutide 0.6 mg, ecnoglutide 1.2 mg, or placebo, all administered subcutaneously once weekly for 24 weeks.
At week 24, HbA1c fell by approximately 1.75 percentage points in the 0.6 mg group and 2.43 percentage points in the 1.2 mg group under the treatment policy estimand, versus a small change in the placebo arm. The proportion of participants reaching HbA1c below 7% was in the range typical for Phase 3 GLP-1 monotherapy studies (roughly 85% or higher on the higher dose). Fasting plasma glucose, postprandial glucose, and body weight all improved dose-dependently. Discontinuation for adverse events was low, and the safety profile was consistent with the class.
The relevant caveat is that a 24-week monotherapy trial in Chinese T2D patients does not tell you how ecnoglutide performs on top of metformin, or against the best available GLP-1 comparator, or in populations with higher baseline HbA1c or established cardiovascular disease. That is what EECOH-2 was designed to address.
EECOH-2: non-inferior to dulaglutide 1.5 mg at 52 weeks, with greater weight loss
EECOH-2 (He et al., Lancet Diabetes Endocrinol 2025, PMID 40854315) is the 52-week, multicenter, open-label, non-inferiority Phase 3 trial that pitted ecnoglutide 0.6 mg and 1.2 mg against dulaglutide 1.5 mg in Chinese T2D patients on metformin monotherapy with elevated glucose. Both ecnoglutide doses met the non-inferiority margin on HbA1c reduction from baseline, and body weight fell more on ecnoglutide than on dulaglutide 1.5 mg.
Dulaglutide is not the toughest comparator in the modern GLP-1 field. Head-to-head reads against semaglutide 1.0 mg (SUSTAIN 7, Pratley et al., Lancet Diabetes Endocrinol 2018, PMID 30122305) and tirzepatide 15 mg (SURPASS-2, Frías et al., NEJM 2021, PMID 34170647) have already shown dulaglutide is not the top of the class. But the EECOH-2 read is still meaningful because it establishes that ecnoglutide clears a real active comparator on both glycemic and weight endpoints in a 52-week Phase 3 with a Chinese T2D population, rather than winning only on placebo comparisons.
SLIMMER-UP-SWITCH: the ecnoglutide vs semaglutide 2.4 mg interim read
The dataset that got the most attention outside China is the SLIMMER-UP-SWITCH head-to-head trial, presented as a late-breaking abstract at the 86th ADA Scientific Sessions in June 2026. This was a multicenter, randomized, open-label Phase 2 study at 17 Chinese sites in 163 adults with obesity, comparing once-weekly ecnoglutide against once-weekly semaglutide at identical 2.4 mg maintenance doses over a planned 60-week treatment period. A pre-specified interim analysis reported at week 20.
At 20 weeks, ecnoglutide 2.4 mg produced a mean body weight change of -12.8% versus -9.5% on semaglutide 2.4 mg (an approximately 35% relative difference in weight reduction at the interim timepoint). Waist circumference dropped about 20% more on ecnoglutide. Responder analyses at week 20 favored ecnoglutide: 99% achieved a 5% or greater loss versus 86% on semaglutide, and 74% achieved a 10% or greater loss versus 40% on semaglutide.
The methodological limitations matter here.
- Interim, not final. Week 20 is early in a 60-week trial. The semaglutide arm, in particular, is still climbing the curve at 20 weeks because the STEP-1 semaglutide 2.4 mg trajectory did not plateau until roughly 60 weeks. The gap at 20 weeks may compress at 60 weeks.
- Open-label. Both arms knew which drug they were on, and both patients and site investigators knew. That is a real bias risk on subjective components of adherence and self-report.
- Chinese population. East Asian adults tend to be lighter at baseline and respond somewhat differently to GLP-1 dosing than Western populations. A 2.4 mg semaglutide dose administered to Chinese adults may not be pharmacokinetically or pharmacodynamically equivalent to the same dose in the STEP trials. Interpret the head-to-head as a within-population comparison, not a universal ranking.
- Not yet peer-reviewed. ADA late-breakers are a conference stage, not a journal read. The full paper has to publish and pass peer review before this interim result can be treated as canonical.
If the 60-week data hold up in a peer-reviewed publication, ecnoglutide would be the first Phase 3 GLP-1 monoagonist to beat semaglutide 2.4 mg on weight endpoints in a head-to-head trial. That is a meaningful "if". Until then, this is a promising signal, not a settled result.
Where ecnoglutide sits in the 2026 GLP-1 field
The peptide receptor pharmacology on ecnoglutide is different from the emerging trends elsewhere in the field. Most next-generation candidates chase multi-receptor agonism: tirzepatide adds GIP to GLP-1, retatrutide adds glucagon on top of that (see the retatrutide triple agonist explainer), survodutide layers glucagon onto GLP-1 (see the survodutide dual-agonist evidence read), and mazdutide runs GLP-1 plus glucagon in Chinese Phase 3. Ecnoglutide instead stays inside a single receptor and tries to do more with it via receptor-level ligand design.
| Candidate | Receptor targets | Mechanism angle | Latest reported weight change | Availability |
|---|---|---|---|---|
| Ecnoglutide 2.4 mg (weekly SC) | GLP-1 | cAMP-biased monoagonist | -16.6% at 48w (SLIMMER Phase 3) | China only (approved Sept 2025) |
| Semaglutide 2.4 mg (weekly SC) | GLP-1 | Full agonist | -14.9% at 68w (STEP-1) | US, EU, UK approved (Wegovy) |
| Tirzepatide 15 mg (weekly SC) | GIP + GLP-1 | Dual agonist | -20.9% at 72w (SURMOUNT-1) | US, EU, UK approved (Zepbound / Mounjaro) |
| Retatrutide 12 mg (weekly SC) | Glucagon + GIP + GLP-1 | Triple agonist | -24.2% at 48w (Phase 2); -28.3% at 80w (TRIUMPH-1 topline) | Investigational |
| Orforglipron 45 mg (daily oral) | GLP-1 | Small molecule oral | -14.7% at 72w (ATTAIN-1) | Investigational |
| Mazdutide 9 mg (weekly SC) | Glucagon + GLP-1 | Dual agonist | -14.8% at 48w (Chinese Phase 3) | Chinese NMPA reviewed |
| Dulaglutide 4.5 mg (weekly SC) | GLP-1 | Full agonist | approximately -6% at 52w (AWARD-11) | US, EU, UK approved (Trulicity) |
Direct cross-trial numeric comparisons like this always overstate certainty because populations, trial lengths, and titration schedules differ. The useful takeaway is not "ecnoglutide beats X" but that a single-receptor GLP-1 monoagonist reaching a placebo-adjusted 15.1% at 48 weeks lands in what used to be dual-agonist territory. Whether that reproduces in Western populations, and whether a longer 68 to 72-week trial widens or narrows the ecnoglutide-semaglutide gap, is unknown.
Safety and tolerability
Adverse event profiles across SLIMMER, EECOH-1, and EECOH-2 were consistent with the GLP-1 class: predominantly gastrointestinal (nausea, diarrhea, constipation, vomiting), mostly mild to moderate, mostly early in titration, and mostly resolving with dose adjustment or time. Discontinuation rates for adverse events on the higher active doses were in the single digits, similar to what has been reported in STEP and SURMOUNT.
The unresolved safety questions cluster in three areas.
Cardiovascular outcomes. Ecnoglutide has secondary reductions in systolic blood pressure, LDL cholesterol, triglycerides, and hs-CRP consistent with weight loss and glycemic improvement. What it does not yet have is a dedicated cardiovascular outcomes trial in the style of SELECT for semaglutide (Lincoff et al., NEJM 2023, PMID 37952131) or SURPASS-CVOT for tirzepatide. Without one, cardiovascular claims for ecnoglutide have to remain at the mechanistic and surrogate-endpoint level.
Thyroid C-cell effects. As a GLP-1 receptor agonist, ecnoglutide carries the same theoretical concern that shows up on the semaglutide and tirzepatide labels: rodent thyroid C-cell tumor findings that have not translated to a confirmed human medullary thyroid carcinoma signal in cohort studies. The Scandinavian cohort study by Pasternak et al. (BMJ 2024, PMID 38580363) did not confirm the C-cell tumor signal in humans on semaglutide. Ecnoglutide has no dedicated long-term thyroid safety cohort of its own, and the label response in China will define the local practice.
Pancreatitis, gallbladder disease, gastroparesis. All GLP-1 receptor agonists have well-catalogued class-level associations with these outcomes at slightly higher rates than comparator therapies. Ecnoglutide has produced no signal outside class expectations in the trials to date, but a Chinese Phase 3 program is not the surveillance apparatus that a US or EU post-marketing dataset would be.
Regulatory status and access
The regulatory picture is compact.
- China (NMPA): Ecnoglutide injection was approved for chronic weight management on 12 September 2025, and separately approved for Type 2 diabetes glycemic control on the basis of EECOH-1 and EECOH-2. It is marketed by Sciwind Biosciences under a Chinese brand name.
- United States: No FDA approval, no active US Phase 3 program registered as of July 2026. Any US clinical use would require an IND-enabled path that has not been announced.
- European Union and United Kingdom: No EMA or MHRA marketing authorization applications reported as of July 2026.
- Peptide research market: Ecnoglutide is not established in the grey-market research-peptide supply chain the way semaglutide, tirzepatide, and retatrutide have become. That may change as the compound moves through more visible development, but as of July 2026 it is not a compound most Western vendors carry. If you are sourcing legitimate research-grade GLP-1 material with a proper certificate of analysis, review our what a peptide COA actually is walkthrough and the Ascension Peptides review for how to think about vendor quality.
For US and EU readers, the immediate translational relevance is limited: you cannot buy ecnoglutide, and there is no Western Phase 3 to enroll in. The reason to pay attention is the mechanism story. If the biased-agonism thesis holds through longer follow-up and a real Western head-to-head, the field will move toward similar receptor-tuning strategies. Sciwind has already opened a Phase 1b/2a of oral ecnoglutide tablets in Chinese participants with overweight or obesity, which would put biased agonism into direct competition with orforglipron, elecoglipron, and other oral small molecule GLP-1s (see the elecoglipron VISTA/SOLSTICE Phase 2 read).
Practical decision framework
If you follow the GLP-1 field for personal, research, or professional reasons, the useful way to hold the ecnoglutide file in your head is the matrix below.
| Question you are asking | What ecnoglutide currently tells you |
|---|---|
| Is there a next-generation GLP-1 monoagonist that competes with semaglutide 2.4 mg on weight loss? | Probably yes, on the strength of SLIMMER Phase 3 and the SLIMMER-UP-SWITCH interim. Peer-reviewed head-to-head at week 60 will decide. |
| Should I expect ecnoglutide to reach the US or EU market soon? | Not on the current regulatory footprint. There is no active Phase 3 in Western populations reported as of July 2026. |
| Is the biased-agonism mechanism a real therapeutic edge or a marketing angle? | Mechanistically plausible and supported by receptor pharmacology; efficacy signal is real; whether the tolerability side of the biased-agonism thesis holds needs longer, larger data. |
| How does ecnoglutide compare to tirzepatide and retatrutide for weight loss? | On current numbers, monoagonist ecnoglutide is closer to semaglutide than to tirzepatide, and it is behind retatrutide's placebo-adjusted range in Phase 2 and TRIUMPH-1 topline. |
| Can I buy or research-inject ecnoglutide? | Not through Western supply chains as of July 2026. It is a China-approved prescription drug, not a research-market peptide. |
For readers thinking about GLP-1 protocols in general, the practical reconstitution and dosing math is compound-independent. If you need the arithmetic on how weekly SC GLP-1 dosing translates from milligram concentration to insulin-syringe units, our reconstitution calculator and the semaglutide dosage chart or tirzepatide dosage chart cover the mechanics that apply to any weekly injectable in this class. And for anyone weighing tirzepatide versus semaglutide on Western-approved compounds, our tirzepatide vs semaglutide 2026 head-to-head guide is a more directly actionable read than a Chinese-only monograph on ecnoglutide.
What actually changed with ecnoglutide
Three things.
First, the biased-agonism approach at the GLP-1 receptor has cleared Phase 3 with a positive obesity and diabetes readout. That was not guaranteed. Prior GPCR bias programs have failed to translate elegant receptor pharmacology into clinical wins.
Second, a Chinese biotech ran a serious head-to-head against semaglutide 2.4 mg and reported a favorable interim without hiding behind a proprietary compound or vague endpoints. Whether the 60-week peer-reviewed read confirms the 20-week signal is the pivotal question for the field.
Third, the Chinese GLP-1 pipeline is now producing compounds that would compete internationally if the regulatory paths existed. Mazdutide, ecnoglutide, and several earlier-stage candidates are being run at Phase 3 scale in populations that Western sponsors historically underserved, and the signal quality is high. That reshapes what the second half of this decade in obesity therapeutics looks like, even if none of these molecules reaches a US pharmacy shelf.
Bottom line: Ecnoglutide is the strongest single-receptor GLP-1 monoagonist story in the field on peer-reviewed Phase 3 numbers alone. It is not yet a Western therapy, not a research peptide most vendors carry, and not head-to-head validated at the 60-week endpoint. What it is, unambiguously, is proof that receptor-level ligand design still has room to move a mature target.
Related reading
- Orforglipron oral GLP-1 Phase 3 evidence 2026
- Mazdutide (IBI362) GLP-1/glucagon dual agonist Phase 3 evidence
- Retatrutide vs tirzepatide vs semaglutide 2026
- Tirzepatide vs semaglutide 2026 head-to-head
- VK2735 (Viking) GLP-1/GIP oral and subcutaneous Phase 2 evidence
- Elecoglipron (AZD5004) VISTA/SOLSTICE oral GLP-1 Phase 2 evidence
- Semaglutide compound page
- Retatrutide compound page
- Ascension Peptides review
- Reconstitution calculator
This article is for educational and research purposes only and is not medical advice. Ecnoglutide (XW003) is a prescription drug approved in China for chronic weight management and Type 2 diabetes and is not approved by the FDA, EMA, or MHRA. All clinical data described above are from Chinese-population Phase 2 and Phase 3 trials (SLIMMER, EECOH-1, EECOH-2, SLIMMER-UP-SWITCH interim) and a conference late-breaker; results in Chinese adults may not generalize to other populations, and the head-to-head against semaglutide reported here is an interim, open-label, not-yet-peer-reviewed analysis. Do not treat cross-trial number-to-number comparisons in this article as a definitive ranking of GLP-1 receptor agonists. GLP-1 receptor agonists share class-level risks including gastrointestinal adverse events, pancreatitis, gallbladder disease, and a boxed thyroid C-cell tumor warning based on rodent data. Any change to diagnosis, monitoring, or treatment of obesity or diabetes should involve a licensed clinician familiar with your medical history.