At a glance
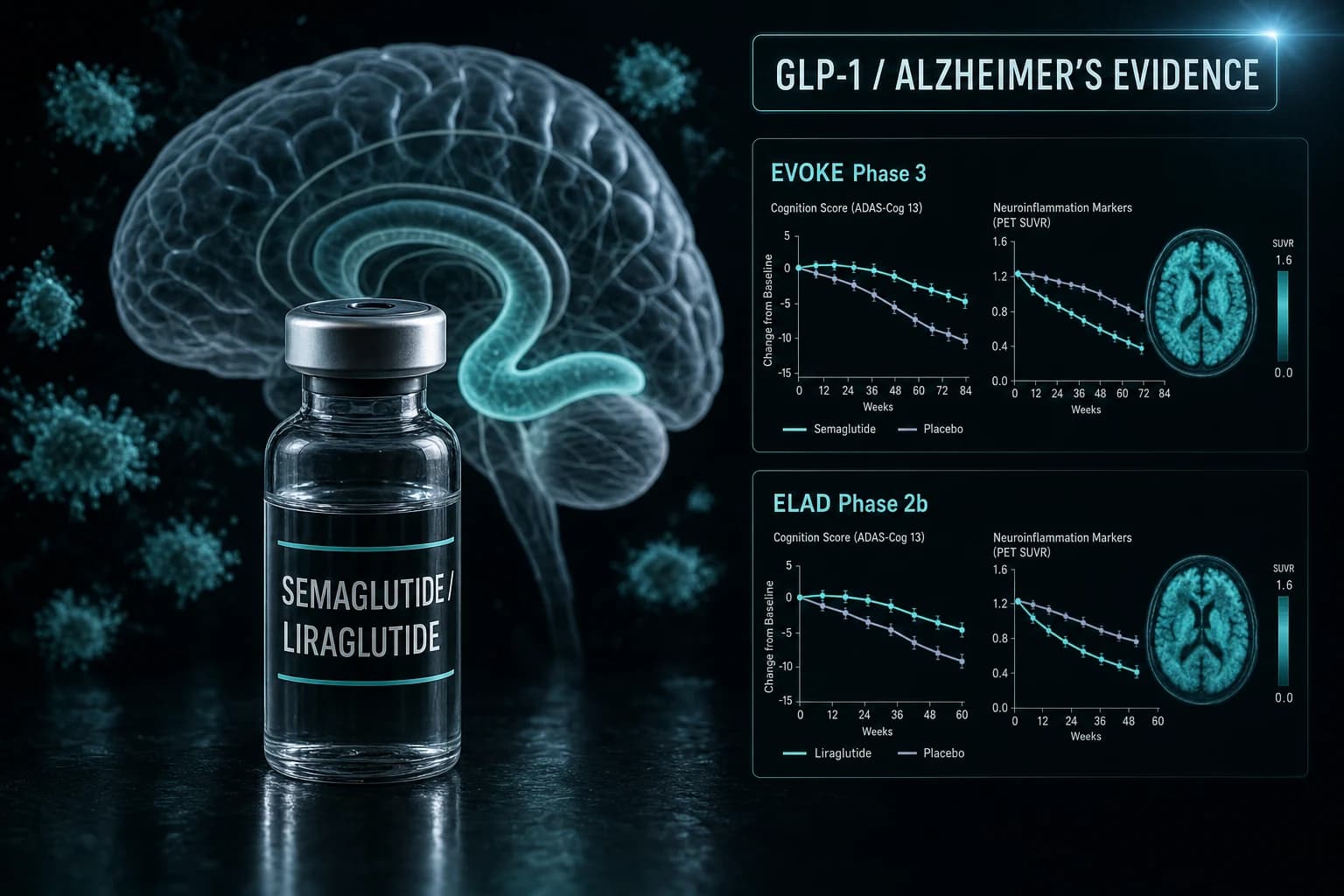
- EVOKE and EVOKE+ Phase 3 (Cummings Lancet 2026, PMID 41865758) missed CDR-SB primary endpoint at week 104 in 3,808 amyloid-positive participants
- ELAD Phase 2b liraglutide (Femminella Nat Med 2025, PMID 41326666) missed CMRglc primary endpoint but reported 50% less gray matter atrophy on MRI
- Gejl 2016 Phase 2 pilot (PMID 27252647) in 38 patients showed preserved CMRglc on liraglutide vs decline on placebo at 26 weeks
- EVOKE moved CSF pTau181, pTau217, total tau, and neurogranin by 7-9% without slowing cognition; plasma NfL rose 5% in EVOKE+
- Wang real-world target trial emulations (PMID 39445596, PMID 40552638) showed 46-70% lower first-time AD diagnoses on semaglutide in type 2 diabetes
- No GLP-1 receptor agonist is FDA approved for Alzheimer's; all clinical use for AD is investigational
A negative Phase 3 in March, biomarkers that moved, and a sober reading
In March 2026, The Lancet published EVOKE and EVOKE+, two Phase 3 trials of oral semaglutide in 3,808 people with early symptomatic Alzheimer's disease. Neither trial slowed clinical progression. The biomarker results were more complicated: CSF phosphorylated tau dropped about 8 to 9 percent, plasma hsCRP dropped roughly 30 percent, and plasma neurofilament light went the wrong way in EVOKE+ (Cummings et al., Lancet 2026, PMID 41865758).
That last detail matters, and most coverage skipped it. So did the smaller liraglutide Phase 2b in Nature Medicine in late 2025, which missed its primary glucose-metabolism endpoint but reported a roughly 50 percent reduction in regional gray matter atrophy (Femminella et al., Nat Med 2025, PMID 41326666).
This article walks through every randomized GLP-1 Alzheimer's trial published to date, what the EVOKE biomarker pattern most plausibly means, and how to read the contradiction between two large real-world observational studies showing a 46 to 70 percent lower dementia diagnosis rate in type 2 diabetes patients on semaglutide (Wang et al., Alzheimers Dement 2024, PMID 39445596).
The complete randomized GLP-1 Alzheimer's record
Four randomized trials. Two drugs. No clinical signal large enough to ground a disease-modifying claim.
| Trial | Year | Drug | Phase | n | Population | Duration | Primary endpoint result |
|---|---|---|---|---|---|---|---|
| Gejl | 2016 | Liraglutide 1.8 mg daily | Phase 2 pilot, double-blind | 38 | Mild AD | 26 weeks | Preserved CMRglc vs decline on placebo; cognition unchanged |
| Femminella (ELAD) | 2025 | Liraglutide 1.8 mg daily | Phase 2b, double-blind | 204 | Mild-to-moderate AD | 52 weeks | CMRglc difference -0.17 (95% CI -0.39 to 0.06), p=0.14 (negative) |
| Cummings (EVOKE) | 2026 | Oral semaglutide up to 14 mg daily | Phase 3, double-blind | 1,855 | Early AD, amyloid+, MCI or mild dementia | 104 weeks | CDR-SB difference -0.08 (95% CI -0.35 to 0.20), p=0.57 (negative) |
| Cummings (EVOKE+) | 2026 | Oral semaglutide up to 14 mg daily | Phase 3, double-blind | 1,953 | Early AD, amyloid+, MCI or mild dementia | 104 weeks | CDR-SB difference 0.10 (95% CI -0.17 to 0.38), p=0.46 (negative) |
Three failed primary endpoints. One pilot too small to call. No randomized trial has yet shown a clinically meaningful slowing of cognitive or functional decline in Alzheimer's with any GLP-1 receptor agonist.
Bottom line: As of mid-2026, no GLP-1 receptor agonist has slowed Alzheimer's progression in a randomized trial. The biggest trial in the class (EVOKE) was negative on its primary endpoint despite moving every plausible biomarker.
Gejl 2016: The pilot that opened the question
The first proper randomized GLP-1 Alzheimer's trial was a 26-week Danish study of 38 patients with mild AD assigned to liraglutide 1.8 mg daily or placebo (Gejl et al., Front Aging Neurosci 2016, PMID 27252647). The primary endpoint was change in cerebral metabolic rate for glucose (CMRglc) on [18F]FDG PET, a sensitive imaging measure of neuronal activity.
Liraglutide-treated patients preserved CMRglc; the placebo group declined. Cognition by WMS-IV did not differ between groups. Amyloid load by [11C]PIB PET increased in temporal cortex in both groups, with no between-group separation.
Two things to keep in mind reading Gejl 2016:
- 38 patients is a pilot. The point was to test feasibility and pick a signal worth chasing.
- CMRglc is a surrogate. It tracks Alzheimer's progression, but moving CMRglc does not in itself prove clinical benefit.
That signal was what motivated the larger ELAD trial.
ELAD 2025: The Phase 2b that failed politely
ELAD (Evaluating Liraglutide in Alzheimer's Disease) was a 52-week Phase 2b at 24 UK sites, 204 patients with mild-to-moderate AD, liraglutide 1.8 mg daily versus placebo (Femminella et al., Nat Med 2025, PMID 41326666).
The primary endpoint, change in CMRglc, missed: estimated difference -0.17 (95% CI -0.39 to 0.06), p=0.14. The trial was negative by its prespecified primary outcome. Two secondary findings drove the headlines anyway:
- Executive cognition on ADAS-Exec favored liraglutide: 0.15-point difference (95% CI 0.03 to 0.28), p=0.01 (unadjusted).
- Liraglutide-treated patients showed roughly 50 percent less gray matter volume loss on MRI in frontal, temporal, parietal, and total gray matter regions.
A 50 percent reduction in atrophy is the kind of number that would, by itself, be exciting if it had been the primary endpoint and survived multiplicity correction. It was neither. Read honestly, ELAD shows that liraglutide does something measurable in the AD brain over a year and does not move the formally tested glucose-metabolism endpoint. The cognition signal was nominal.
EVOKE and EVOKE+ 2026: The Phase 3 that closed most of the question
EVOKE and EVOKE+ were identical, parallel Phase 3 trials at 566 sites in 40 countries, randomizing 3,808 amyloid-positive participants (1,855 in EVOKE, 1,953 in EVOKE+), ages 55 to 85, with MMSE at least 22, to oral semaglutide titrated up to 14 mg daily or placebo for 104 weeks (Cummings et al., Lancet 2026, PMID 41865758; design paper Cummings et al., Alzheimers Res Ther 2024, PMID 39780249).
The primary endpoint was change in CDR-SB at week 104. Mean CDR-SB change was 2.3 with semaglutide vs 2.3 with placebo in EVOKE (estimated difference -0.08, 95% CI -0.35 to 0.20, p=0.57) and 2.2 vs 2.1 in EVOKE+ (estimated difference 0.10, 95% CI -0.17 to 0.38, p=0.46).
Treatment-emergent adverse events occurred in 91.2 percent of semaglutide patients vs 84.8 percent of placebo patients, consistent with semaglutide's known GI profile in other indications. No new safety signal emerged in this older AD population.
This is the largest GLP-1 trial ever run for any neurodegenerative disease. It was negative on its primary endpoint.
The biomarker pattern that complicates the negative read
If EVOKE were entirely negative, the story would be straightforward. It is not.
In the semaglutide arm at week 104:
- CSF pTau181 fell to a treatment ratio of 0.92 vs placebo (about 8 percent lower).
- CSF pTau217 fell to 0.91.
- CSF total tau fell to 0.93.
- CSF neurogranin (a synaptic marker) fell to 0.92.
- CSF YKL-40 (neuroinflammation) fell to 0.93.
- Plasma hsCRP fell roughly 30 percent.
These are biomarkers that move with disease activity. Lecanemab and donanemab, which are FDA approved for early AD, slow CDR-SB decline by about 25 to 35 percent and move similar tau biomarkers. EVOKE moved the biomarkers without slowing CDR-SB at all.
One signal cut the other way. Plasma neurofilament light chain (NfL), a marker of axonal damage, rose roughly 5 percent in EVOKE+ (treatment ratio 1.05, 95% CI 1.01 to 1.08). That is a small move in the wrong direction in a population where NfL ordinarily rises with progression. Researchers presenting at CTAD 2025 flagged it as the most concerning EVOKE finding, not the headline CDR-SB miss.
Note: Moving CSF tau without moving cognition is not unprecedented in AD trials. Several gamma-secretase modulators did the same in the 2010s. The current best interpretation is that some pathways gate downstream cognitive change and others do not.
The real-world data: where the 70 percent figure comes from
Two large observational analyses by Wang and colleagues used target trial emulation on US electronic health records to compare semaglutide with other antidiabetic drugs in type 2 diabetes:
- The first paper, Wang et al., Alzheimers Dement 2024, PMID 39445596, reported 40 to 70 percent lower first-time AD diagnoses in semaglutide users vs comparators across seven different reference drugs.
- The follow-up, Wang et al., J Alzheimers Dis 2025, PMID 40552638, expanded to all Alzheimer's disease-related dementias (ADRD): hazard ratio 0.54 (95% CI 0.49 to 0.59) vs insulin, with smaller advantages vs metformin and older GLP-1s.
These are well-executed target trial emulations on a 1.7 million-patient cohort. They are not Phase 3 evidence. They are observational, so unmeasured confounders (cardiovascular risk, body weight trajectory, healthcare utilization, GLP-1 prescribing patterns) cannot be ruled out. They also study a different question: prevention or delay of dementia onset in metabolically unwell patients, not slowing of progression in established AD.
That distinction explains most of the apparent EVOKE contradiction. Wang et al. asked whether semaglutide changes who gets diagnosed. EVOKE asked whether semaglutide changes the course of disease that is already diagnosed. Both can be true at once: a treatment can shift incidence in a metabolic population and do nothing in an amyloid-positive, post-diagnosis population.
Why GLP-1 was a candidate at all
GLP-1 receptors are expressed in hippocampal, cortical, and hypothalamic neurons. Preclinical AD models, in transgenic mice and in cell cultures, have shown that GLP-1 agonism reduces amyloid plaque burden, decreases tau phosphorylation, restores hippocampal long-term potentiation, and improves spatial memory. The peripheral mechanisms (insulin sensitization, weight loss, vascular inflammation reduction) overlap with known AD risk factors. None of that translation should have been taken for granted, and EVOKE was the appropriate test.
EVOKE's failure narrows the hypothesis. Cognitive benefit in established Alzheimer's, in an amyloid-confirmed population, on a 2-year horizon, with the most clinically validated oral GLP-1 dose, is unlikely to come from semaglutide alone. The class question (different drug, earlier disease, prevention design) remains open.
What is still in flight
Several adjacent questions are still being tested:
- A dulaglutide trial in mild cognitive impairment with cognitive endpoints is enrolling.
- Tirzepatide AD trials have been discussed publicly but no large Phase 3 readout has been published.
- Subgroup analyses from EVOKE looking at APOE4 carriers, baseline tau load, and BMI are being prepared for AD/PD 2026 and CTAD 2026.
- A planned analysis is investigating whether the biomarker effect translates over longer follow-up.
If you are tracking the GLP-1 class for non-AD indications, see our companion piece on GLP-1s for Parkinson's, where LIXIPARK and Exenatide-PD3 told a similar story, and the SUMMIT Phase 3 tirzepatide HFpEF program.
How to read this in the broader GLP-1 indication map
The class context matters because Alzheimer's is the third major non-obesity indication tested for GLP-1 in 2024-2026 (after MASH and Parkinson's), and the second to miss its primary endpoint.
| Indication | Pivotal trial | Result |
|---|---|---|
| Obesity | STEP, SURMOUNT, SURPASS, TRIUMPH | Established |
| Type 2 diabetes | SUSTAIN, SURPASS | Established |
| Cardiovascular | SELECT, REWIND | Positive (semaglutide, dulaglutide) |
| Sleep apnea | SURMOUNT-OSA | Positive (tirzepatide) |
| HFpEF | SUMMIT | Positive (tirzepatide) |
| MASH | ESSENCE | Positive (semaglutide) |
| Knee osteoarthritis | TRIUMPH-4 | Positive (retatrutide topline) |
| Parkinson's | LIXIPARK, Exenatide-PD3 | Mixed (Phase 2 positive, Phase 3 negative) |
| Alzheimer's | EVOKE, EVOKE+ | Negative |
GLP-1s look genuinely systemic in obesity, cardiometabolic disease, and weight-mediated conditions. They look uncertain in primary neurodegenerative disease.
For researchers tracking semaglutide more broadly, our coverage of the ESSENCE MASH Phase 3 readout and the stopping-GLP-1 weight regain literature covers indications where the evidence held up. For oral GLP-1 evidence in metabolic disease, see the orforglipron Phase 3 review. For the broader class comparison, see tirzepatide vs semaglutide head-to-head 2026 and the GLP-1 muscle loss evidence review.
Bottom line: EVOKE moved several Alzheimer's biomarkers by 7 to 9 percent and CSF pTau in particular by a clinically interesting amount, but it did not move cognition or function over two years. Until a future trial shows that those biomarker shifts translate, oral semaglutide is not an Alzheimer's drug.
The honest reading
The EVOKE result is not ambiguous on its primary endpoint. Both trials missed. Biomarkers moved in the direction one would predict for a disease-modifying agent, but cognition did not.
There are three reasonable interpretations and one bad one.
- Interpretation A: GLP-1 agonism modulates AD biology without altering the dominant drivers of post-diagnosis decline. This is consistent with EVOKE and with the Wang prevention signal both being true.
- Interpretation B: The trial was on the wrong patients. Amyloid-positive, MCI or mild dementia is a late point at which to expect a metabolic intervention to bend disease trajectory. The next generation of GLP-1 AD trials may need to enroll earlier (preclinical AD, APOE4 carriers, type 2 diabetes with cognitive risk).
- Interpretation C: 14 mg oral semaglutide hit a maximum tolerated peripheral exposure but a sub-therapeutic central exposure. Injectable semaglutide reaches higher plasma levels at clinically approved doses. EVOKE did not test that.
- The bad interpretation: ignore EVOKE and keep citing the Wang observational data as if it were Phase 3 evidence. It is not. Reading anything as randomized evidence that is not randomized evidence is the easiest mistake to make in this space.
For now, the verifiable answer is the cautious one. No GLP-1 receptor agonist is an Alzheimer's treatment in 2026. Several are interesting candidates for prevention research that has not yet been done.
Researchers studying tirzepatide or semaglutide for non-AD endpoints can find clinician-vetted vials at Ascension Peptides with code ENHANCED for 50 percent off injectables. For oral peptides on the metabolic side, Limitless Biotech offers research-grade orals with code ENHANCED.
References
- Cummings J, et al. Efficacy and safety of oral semaglutide 14 mg (flexible dose) in early-stage symptomatic Alzheimer's disease (evoke and evoke+): two phase 3, randomised, placebo-controlled trials. Lancet. 2026. PMID 41865758
- Cummings J, et al. evoke and evoke+: design of two large-scale, double-blind, placebo-controlled, phase 3 studies evaluating efficacy, safety, and tolerability of semaglutide in early-stage symptomatic Alzheimer's disease. Alzheimers Res Ther. 2025;17(1):8. PMID 39780249
- Femminella GD, et al. Liraglutide in mild to moderate Alzheimer's disease: a phase 2b clinical trial. Nat Med. 2025. PMID 41326666
- Gejl M, et al. In Alzheimer's Disease, 6-Month Treatment with GLP-1 Analog Prevents Decline of Brain Glucose Metabolism: Randomized, Placebo-Controlled, Double-Blind Clinical Trial. Front Aging Neurosci. 2016;8:108. PMID 27252647
- Wang W, et al. Associations of semaglutide with first-time diagnosis of Alzheimer's disease in patients with type 2 diabetes: Target trial emulation using nationwide real-world data in the US. Alzheimers Dement. 2024. PMID 39445596
- Wang W, et al. Associations of semaglutide with Alzheimer's disease-related dementias in patients with type 2 diabetes: A real-world target trial emulation study. J Alzheimers Dis. 2025. PMID 40552638
This article is for educational and research purposes only. None of the content above constitutes medical advice. Semaglutide is FDA approved as Ozempic for type 2 diabetes, as Wegovy for chronic weight management, and as Rybelsus for type 2 diabetes; it is not approved for Alzheimer's disease. Decisions about Alzheimer's care belong with the patient, family, and treating neurologist or geriatrician.