At a glance
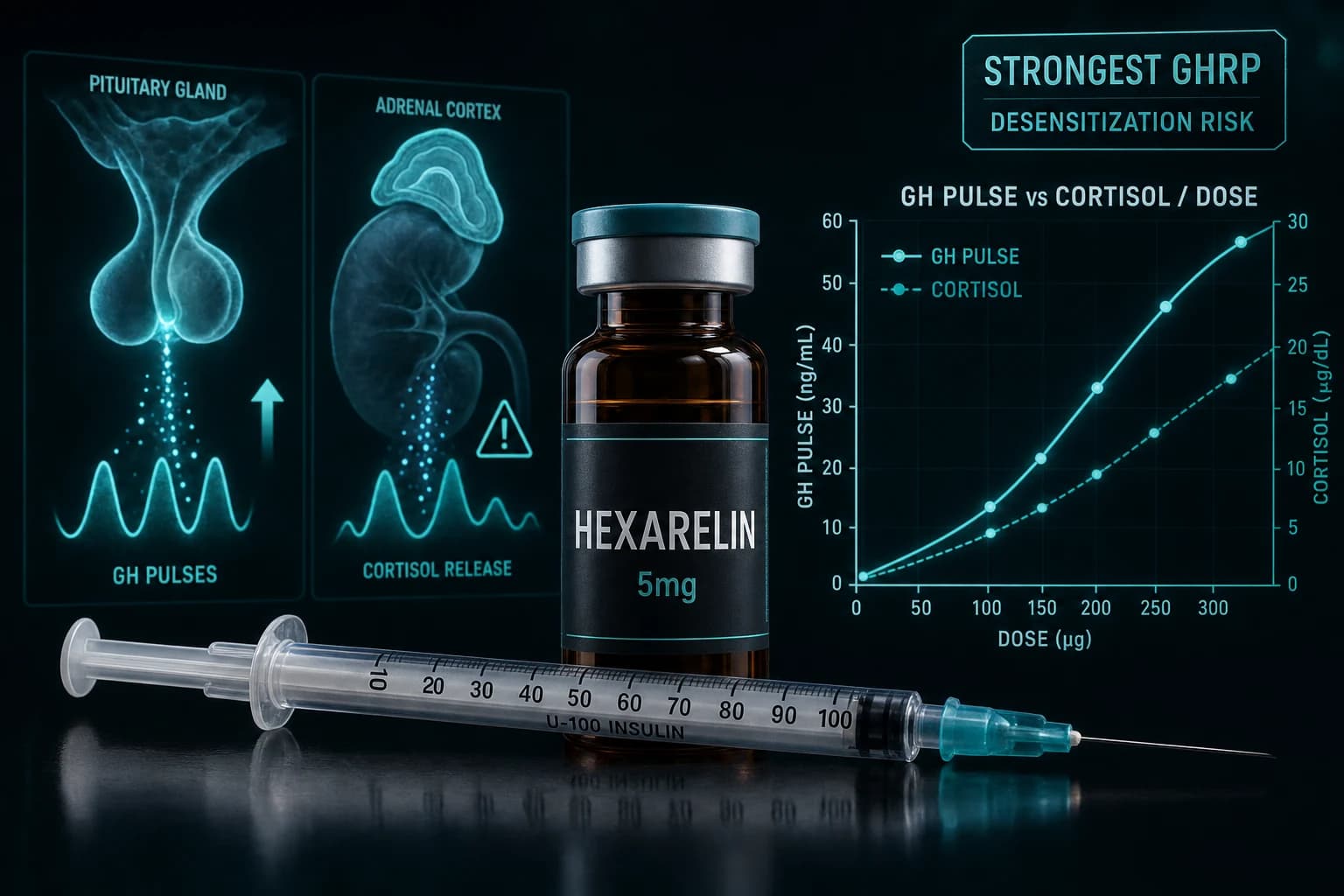
- Hexarelin is a synthetic hexapeptide GHRP with the strongest GH-releasing activity of the GHRP class (stronger than GHRP-2, GHRP-6, and Ipamorelin)
- Standard research dose: 100 mcg subcutaneous 1-3 times daily; cycles capped at 4-6 weeks to avoid desensitization and cortisol elevation
- Unlike Ipamorelin, hexarelin produces measurable elevation of cortisol and prolactin at standard doses; this is the primary safety differentiator
- Cardio-protective effects independent of GH release have been characterized in rodent and limited human studies (Tivesten et al., 1999)
- Pairs with a GHRH analog (CJC-1295 or Sermorelin) in the classic GHRP + GHRH stack structure for synergistic GH pulse amplification
Hexarelin is the GHRP nobody runs casually. It is the strongest GH releaser in the class, capable of producing GH pulses that match or exceed clinical GH dosing in some research contexts. The trade-off is real: hexarelin also elevates cortisol and prolactin at standard doses, and desensitization develops more aggressively than with weaker GHRPs like Ipamorelin. The compound has a defined research role for short, targeted GH-pulse cycles where maximum amplitude matters, but it is not the default choice for general body composition work.
This article covers what hexarelin actually is, the GH-release potency that distinguishes it, the cortisol and prolactin elevation that constrains its use, the standard research protocols, and how it compares to the cleaner-mechanism alternatives like Ipamorelin and the CJC-1295/Ipamorelin combination.
What hexarelin actually is
Hexarelin is a synthetic hexapeptide (6 amino acids) belonging to the growth hormone releasing peptide (GHRP) class. Like other GHRPs, it activates the GHSR-1a (ghrelin receptor) in the anterior pituitary to drive growth hormone release. The molecular sequence is His-D-2-methyl-Trp-Ala-Trp-D-Phe-Lys-NH2, with chemical modifications that increase potency relative to natural ghrelin and other GHRPs.
| Property | Hexarelin value |
|---|---|
| Sequence | 6 amino acids (hexapeptide) |
| Receptor | GHSR-1a (ghrelin receptor) |
| Mechanism | Pituitary GH release via GHSR-1a activation |
| Class | GHRP (growth hormone releasing peptide) |
| Half-life | Short (minutes to a few hours circulating) |
| Route | Subcutaneous, IM, or IV |
| Strongest competing GHRPs | GHRP-2, GHRP-6, Ipamorelin |
The original characterization of hexarelin's GH-stimulating potency in humans came from Ghigo et al., Eur J Endocrinol, 1995, which demonstrated reproducible GH release in healthy subjects. Subsequent work by Imbimbo et al., Clin Endocrinol, 1994 characterized the dose-response relationship and confirmed potent GH release at low doses.
GH-release potency: how hexarelin compares
Across the GHRP class, hexarelin sits at the top of the potency hierarchy:
| GHRP | Relative GH potency | Cortisol effect | Prolactin effect |
|---|---|---|---|
| Hexarelin | Strongest | Modest elevation | Modest elevation |
| GHRP-2 | Strong | Mild elevation | Mild elevation |
| GHRP-6 | Strong (with hunger sx) | Mild elevation | Mild elevation |
| Ipamorelin | Moderate | Minimal | Minimal |
In comparative head-to-head testing, hexarelin produces larger and more reliable GH pulses than the other GHRPs at matched doses. The mechanism explanation: hexarelin has higher GHSR-1a affinity and binding stability than other GHRP class members, producing more sustained receptor activation per injection.
The downside is what comes with that stronger activation. The GHSR-1a is not exclusively involved in GH release. It also influences cortisol secretion through adrenocorticotropic hormone (ACTH) effects and produces prolactin elevation through related pathways. The same potency that drives hexarelin's GH advantage drives its off-target effects.
For mechanism context, Massoud et al., Clin Endocrinol, 1996 characterized hexarelin's hypothalamic-pituitary-adrenal axis effects in detail.
The cortisol and prolactin issue
Hexarelin elevates cortisol meaningfully at clinical-grade doses. The elevation pattern:
- Acute (first few hours after injection): Cortisol can rise 50-100% above baseline at standard research doses (100 mcg SC)
- Daily integration: Multiple-times-daily dosing produces cumulatively elevated cortisol exposure across the day
- Chronic: Long cycles (beyond 4-6 weeks) may produce sustained cortisol elevation patterns
For comparison, Ipamorelin produces essentially no measurable cortisol elevation at clinical doses. This is the central differentiator between the two compounds. Researchers running protocols where cortisol elevation is undesirable (most metabolic, body composition, and recovery research) generally prefer Ipamorelin.
Prolactin elevation is also documented but is typically smaller in magnitude than the cortisol effect.
Bottom line: Hexarelin's strength is also its constraint. Maximum GH-release potency comes with measurable cortisol and prolactin elevation that Ipamorelin avoids. The choice between them depends on whether the research goal prioritizes peak GH amplitude or clean GH mechanism.
The desensitization issue
GHSR-1a receptors undergo desensitization with sustained ligand exposure. With hexarelin, the desensitization develops more aggressively than with weaker GHRPs:
| Timeline | Hexarelin response pattern |
|---|---|
| Days 1-7 | Full GH pulse amplitude on each injection |
| Weeks 2-3 | Modestly reduced amplitude; tachyphylaxis beginning |
| Weeks 4-6 | Substantially reduced response; clinical effect waning |
| Beyond 6 weeks | Largely desensitized; longer washouts required to restore response |
This is why most hexarelin research protocols cap cycles at 4-6 weeks with extended washout periods between cycles. Longer continuous exposure does not produce continued benefit and may produce sustained off-target effects.
For the Cardio context, Tivesten et al., Am J Physiol, 1999 characterized cardio-protective effects of hexarelin that appear to operate independently of GH release. These effects may persist somewhat longer than the GH-pulse effects, but the trial designs were small.
The standard research protocol
Across published clinical-grade studies and forum-documented research protocols, the convergent dosing:
| Phase | Dose | Frequency | Timing | Duration |
|---|---|---|---|---|
| Standard research | 100 mcg | 1-3 times daily, SC | Pre-meal or pre-bed | 4-6 weeks |
| Conservative | 100 mcg | Once daily, SC | Pre-bed | 4-6 weeks |
| Aggressive (with caveats) | 200 mcg | 2-3 times daily, SC | Distributed | 4 weeks |
| Localized injection (research) | 50-100 mcg | Once daily, SC near target | 4 weeks |
Three reasons most protocols cap dose at 100 mcg per injection:
-
GH pulse saturation. Doses above 100 mcg do not produce proportionally larger GH pulses because receptor binding approaches saturation. Diminishing returns set in quickly.
-
Cortisol scales with dose. While GH effect saturates, cortisol elevation continues to rise with dose. The risk-benefit math favors lower doses.
-
Desensitization accelerates with higher doses. Higher per-injection doses appear to accelerate the tachyphylaxis timeline.
Pairing with a GHRH analog
The classic GHRP + GHRH stack pairs hexarelin (or another GHRP) with a GHRH analog (CJC-1295 or Sermorelin). The mechanism rationale:
- GHRPs (hexarelin) work through GHSR-1a to release GH and amplify GHRH-driven release
- GHRH analogs (CJC-1295) work through GHRH receptor to stimulate native GH production
- Combined, the two pathways amplify each other beyond either acting alone
| Stack option | Dose | Note |
|---|---|---|
| Hexarelin + CJC-1295 (no DAC) | 100 mcg each, 1-3x daily | Strongest combined pulse |
| Hexarelin + Sermorelin | 100 mcg + 200-500 mcg, daily | Cleaner pulse profile |
| Ipamorelin + CJC-1295 | 100 mcg each, 1-3x daily | The "FIT Stack" alternative |
The FIT Stack (CJC-1295 + Ipamorelin) is the cleaner-mechanism version of this approach without the cortisol/prolactin overhead. For most research applications, the FIT Stack delivers most of the GH-pulse benefit without the hexarelin trade-offs. Hexarelin is the right choice when maximum GH amplitude is the specific research priority.
For comparison context, see the Sermorelin vs CJC-1295 vs Ipamorelin comparison and the FIT Stack CJC-1295 + Ipamorelin GH protocol.
When hexarelin is the right choice
Three research contexts where hexarelin specifically (not Ipamorelin) makes sense:
1. Maximum-amplitude GH pulse research. When the research question requires the largest possible single-injection GH pulse, hexarelin produces measurably more GH than Ipamorelin or other GHRPs. The cortisol overhead is accepted as a necessary trade-off.
2. Short cycle interventions. Hexarelin's faster desensitization makes it appropriate for short-cycle research (2-4 weeks) where the goal is intense GH stimulation over a defined window, not long-term sustained release.
3. Cardio-protection research. The cardio-protective effects characterized by Tivesten and others may be specific to hexarelin's particular receptor binding profile and may not generalize across the GHRP class. Research targeting cardiac endpoints may specifically choose hexarelin for this reason.
For most other research goals (general body composition, recovery, GH support without cortisol concerns, longer cycles), Ipamorelin or the FIT Stack is the cleaner default.
Safety considerations
Beyond cortisol and prolactin elevation, hexarelin's safety profile in published trials includes:
Injection-site reactions. Mild and transient at standard doses.
Glucose elevation. Acute injections produce transient hyperglycemia consistent with GH pulse effects.
Insulin resistance (chronic concern). Sustained GH elevation contributes to insulin resistance. The 4-6 week cycle cap is partly aimed at this.
Fluid retention. Common with all GH-pulse-driving compounds; typically mild and resolves on cycle cessation.
Hunger (less than GHRP-6). Hexarelin produces less appetite stimulation than GHRP-6 but more than Ipamorelin.
Patients with diabetes, uncontrolled hypertension, or active malignancy should not use hexarelin. The compound is not appropriate for pregnancy or breastfeeding contexts.
How hexarelin fits the 2026 regulatory landscape
Hexarelin was not among the 14 peptides reclassified to Category 1 in the Feb 27, 2026 HHS announcement. It remains a research compound without compounding-pharmacy access through standard 503A pathways. Research-grade retail availability through peptide vendors continues to be the practical channel.
For the broader regulatory context, see the FDA peptide reclassification February 2026 complete breakdown.
Sourcing
For research-grade injectable hexarelin, Ascension Peptides carries it in the GH secretagogue catalog with public per-batch COAs and 50% off using code ENHANCED. For our broader sourcing analysis, see the best legit peptide vendors 2026 ranking.
FAQ
What is hexarelin?
Hexarelin is a synthetic hexapeptide (6 amino acids) growth hormone releasing peptide (GHRP). It activates the GHSR-1a (ghrelin receptor) in the pituitary to drive GH release. Among the GHRP class, hexarelin produces the largest GH pulses but also has more measurable cortisol and prolactin elevation than weaker alternatives like Ipamorelin.
Is hexarelin better than Ipamorelin?
For GH-pulse amplitude, yes. For cortisol-free GH stimulation, no. The choice depends on research goal. Maximum-amplitude GH research favors hexarelin; clean-mechanism body composition and recovery research favors Ipamorelin.
What is the standard hexarelin research dose?
100 mcg subcutaneous 1-3 times daily for 4-6 week cycles. Higher per-injection doses do not produce proportionally larger GH pulses due to receptor binding saturation, but do produce more cortisol elevation.
Why does hexarelin cause cortisol elevation?
GHSR-1a (ghrelin receptor) activation produces effects beyond GH release, including ACTH stimulation that drives cortisol production. Hexarelin's higher GHSR-1a affinity produces both the stronger GH effect and the larger off-target cortisol effect. Ipamorelin's lower affinity and different binding profile produces less cortisol elevation.
How long should I run a hexarelin cycle?
4-6 weeks is the typical cap. Beyond this window, GHSR-1a desensitization substantially reduces the GH pulse response, making continued dosing unproductive. Extended washouts (4-8 weeks off-cycle) between hexarelin cycles allow receptor sensitivity to recover.
Can I stack hexarelin with CJC-1295?
Yes, this is the classic GHRP + GHRH stack structure. The combination amplifies GH pulses beyond either compound alone. The trade-off versus the cleaner FIT Stack (CJC-1295 + Ipamorelin) is cortisol elevation; hexarelin produces more cortisol than Ipamorelin in this combination.
Is hexarelin safe?
In published clinical-grade studies at standard doses, hexarelin has been generally well-tolerated short-term. Long-term safety is less characterized. The cortisol elevation, prolactin elevation, and insulin resistance concerns scale with dose and duration. The compound is not appropriate for patients with diabetes, uncontrolled hypertension, active malignancy, or in pregnancy/breastfeeding contexts.
Further reading
- Sermorelin vs CJC-1295 vs Ipamorelin comparison
- FIT Stack CJC-1295 + Ipamorelin GH protocol
- IGF-1 LR3 research dosing protocol
- MK-677 (Ibutamoren) oral GH secretagogue guide
- CJC-1295 + Ipamorelin stack protocol
- Best legit peptide vendors 2026
- Reconstitution Calculator
This article is for educational and research purposes only. Hexarelin is sold under research-use disclosures and is not approved by the FDA for any indication. None of the content above constitutes medical advice. Consult a qualified clinician for individual medical questions about growth hormone research or related conditions.


