At a glance
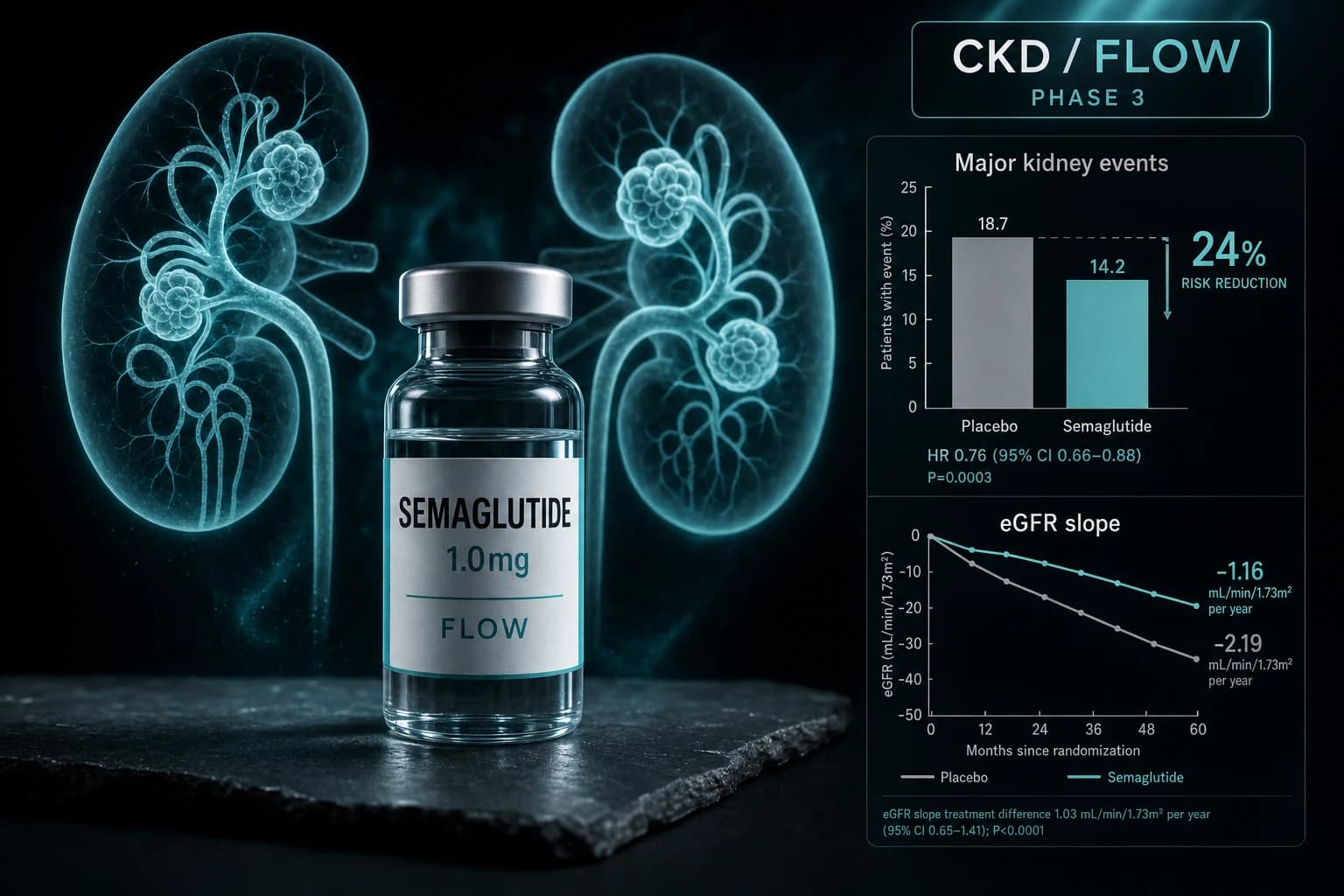
- FLOW Phase 3 (Perkovic NEJM 2024, PMID 38785209) cut major kidney events by 24% in 3,533 adults with T2D and CKD
- MACE fell 18%, all-cause death fell 20%, HF outcomes fell 27% on once-weekly semaglutide 1.0 mg
- eGFR slope was 1.16 mL/min/1.73 m^2 less steep per year vs placebo over median 3.4 year follow-up
- Benefit held regardless of background SGLT2 inhibitor (Mann Nat Med 2024, PMID 38914124) or CKD severity
- Trial stopped early for efficacy in October 2023 on the recommendation of the independent DMC
- Semaglutide is not FDA approved for CKD; this is a research and clinical-practice update, not a label change
A Phase 3 stopped early for efficacy, and a 24% kidney result that changed the GLP-1 indication map
In October 2023, Novo Nordisk's independent Data Monitoring Committee told the company to stop the FLOW trial. Not because semaglutide was hurting people. Because the kidney endpoint had already separated from placebo enough that continuing the trial was no longer ethical. Seven months later, the full results landed in NEJM (Perkovic et al., NEJM 2024, PMID 38785209).
The primary outcome, a five-component composite of major kidney disease events and death from kidney or cardiovascular causes, fell by 24 percent (HR 0.76, 95% CI 0.66 to 0.88, p=0.0003) in 3,533 adults with type 2 diabetes and chronic kidney disease over a median 3.4 years of follow-up. Major cardiovascular events fell 18 percent. All-cause death fell 20 percent. The trial added GLP-1 receptor agonism to the very short list of drug classes shown to slow diabetic kidney disease in a dedicated Phase 3, alongside SGLT2 inhibitors and the nonsteroidal MRA finerenone.
This article walks through what FLOW actually found, who was in it, how the result holds up after the SGLT2-inhibitor subgroup analysis, the heart failure analysis, the CKD severity stratification, and what the data does and does not say about adding semaglutide to a modern nephrology regimen.
What FLOW measured and why the primary outcome matters
FLOW (NCT03819153) was a randomised, double-blind, placebo-controlled, multinational Phase 3b trial. Eligibility was the same set of CKD definitions clinical nephrologists use to identify patients at elevated risk of progression (Rossing et al., Nephrol Dial Transplant 2023, PMID 36651820):
- eGFR 50 to 75 mL/min/1.73 m^2 with UACR 300 to 5,000 mg/g, or
- eGFR 25 to less than 50 mL/min/1.73 m^2 with UACR 100 to 5,000 mg/g.
Background therapy required renin-angiotensin-aldosterone system blockade (ACE inhibitor or ARB) at maximum tolerated dose unless contraindicated. SGLT2 inhibitors were permitted but not required. Participants were randomised 1:1 to subcutaneous semaglutide 1.0 mg once weekly or matched placebo.
The primary outcome was a five-component composite: persistent eGFR decline of 50 percent or more from baseline, persistent eGFR below 15 mL/min/1.73 m^2, initiation of chronic kidney replacement therapy (dialysis or transplant), death from kidney disease, or death from cardiovascular disease. This is a standard "major kidney disease event" composite that mirrors what was used in DAPA-CKD and EMPA-KIDNEY for SGLT2 inhibitor trials.
Note: "eGFR 25 to under 50" reaches into CKD stage 4. Most nephrology trials are restricted to stage 3. FLOW deliberately included a more advanced kidney population, which made the eventual safety and efficacy result across the severity spectrum more interpretable.
Who was in FLOW
The 3,533 randomised participants were not lightly affected. Baseline mean age 66.6, mean HbA1c 7.8 percent, mean diabetes duration 17.4 years, mean eGFR 47 mL/min/1.73 m^2, median UACR 568 mg/g, and 68.2 percent classified as very high risk for CKD progression by KDIGO criteria. About 15.6 percent were already on an SGLT2 inhibitor at baseline.
This is the population most nephrologists encounter at a diabetic kidney disease clinic: not screen-detected disease, established CKD with substantial albuminuria, on full-dose RAAS blockade, often with one comorbid cardiovascular event already on the chart.
The headline result
Over 3.4 years of median follow-up, the primary composite event rate was 5.8 per 100 patient-years on semaglutide and 7.5 per 100 patient-years on placebo. Hazard ratio 0.76. The hierarchical secondary outcomes followed.
| Endpoint | Semaglutide vs placebo | Hazard ratio (95% CI) | p value |
|---|---|---|---|
| Primary composite (major kidney events + kidney/CV death) | 5.8 vs 7.5 per 100 PY | 0.76 (0.66 to 0.88) | 0.0003 |
| Annual eGFR slope | Difference 1.16 mL/min/1.73 m^2/year less steep | n/a | <0.001 |
| Major adverse cardiovascular events (MACE) | 5.1 vs 6.2 per 100 PY | 0.82 (0.68 to 0.98) | 0.029 |
| All-cause death | n/a | 0.80 (0.67 to 0.95) | 0.01 |
Every confirmatory secondary tested in the hierarchy reached statistical significance, which is unusual. Many cardio-renal trials show a primary endpoint signal that does not propagate to mortality. FLOW did.
The eGFR slope number deserves attention. A 1.16 mL/min/1.73 m^2 per year difference, sustained over 3.4 years, translates to roughly 4 mL/min/1.73 m^2 of preserved kidney function across the trial. In a population starting at 47 mL/min/1.73 m^2, that is the difference between staying in stage 3 and moving to stage 4 over the same observation window for many patients.
Heart failure: the underappreciated FLOW result
Most coverage of FLOW emphasised the kidney composite. The heart failure data from the prespecified analysis is the second story.
Pratley et al., JACC 2024, PMID 39217553 reported the FLOW heart failure outcomes. The composite of first heart failure event or cardiovascular death fell 27 percent on semaglutide. Heart failure events alone fell 27 percent. Cardiovascular death fell 29 percent.
This matters because the FLOW cohort overlaps significantly with the population SGLT2 inhibitors target, and with the population in which tirzepatide showed Phase 3 benefit for HFpEF in the SUMMIT trial. The GLP-1 class now has independent randomised evidence for slowing CKD progression and for reducing heart failure events in CKD+diabetes, on top of the obesity-related HFpEF signal from the STEP-HFpEF program. That is a coherent cardiometabolic story rather than a single-organ result.
The SGLT2 inhibitor question
The first question every nephrologist asked after FLOW was whether the kidney benefit would survive in patients already on an SGLT2 inhibitor. SGLT2s are now standard of care for diabetic kidney disease. If FLOW only worked in SGLT2-naive patients, the practical impact would be limited.
Mann et al., Nat Med 2024, PMID 38914124 addressed this directly in a prespecified subgroup analysis. Of the 3,533 randomised participants, 550 were on an SGLT2 inhibitor at baseline. The kidney, cardiovascular, and mortality benefits of semaglutide did not differ statistically by SGLT2 status. The point estimates were consistent.
That is the most useful finding for clinical decision-making. It suggests semaglutide adds independently to SGLT2 inhibition rather than substituting for it, which is what the mechanistic literature would predict because the two classes hit different pathways (proximal tubule sodium-glucose cotransport vs central appetite regulation, weight, glycemia, and vascular inflammation).
CKD severity: does the benefit attenuate at lower eGFR?
A separate prespecified analysis stratified outcomes by baseline CKD severity (FLOW CKD severity analysis, kidney/survival, 2026, PMID 41706532, and cardiovascular by CKD severity, Eur Heart J 2024, PMID 39211948).
The kidney and survival benefit held across the eGFR and UACR spectrum, including participants who entered with advanced CKD. The cardiovascular benefit also held, with no significant interaction by CKD severity. Practically, that means a patient with eGFR 30 mL/min/1.73 m^2 and UACR 1,000 mg/g and a patient with eGFR 60 mL/min/1.73 m^2 and UACR 400 mg/g both gained from semaglutide in FLOW.
Bottom line: Across the SGLT2 inhibitor and CKD severity subgroups, the FLOW benefit was preserved. The trial does not appear to depend on a narrow phenotype.
Mechanism: what is semaglutide doing in the kidney?
FLOW is an outcomes trial, not a mechanism paper. It cannot tell us why semaglutide preserved eGFR. But the magnitude of the eGFR slope effect (1.16 mL/min/1.73 m^2/year) is larger than what would be expected from HbA1c and weight reduction alone, based on the SUSTAIN and STEP trial datasets. That implies at least part of the kidney benefit is mediated independently of glycemia and weight.
The candidate mechanisms, drawing on preclinical literature and FLOW's biomarker substudies, include:
- Reduced glomerular hyperfiltration through tubuloglomerular feedback restoration.
- Lower intraglomerular pressure via efferent arteriolar effects.
- Reduced renal inflammation and oxidative stress; semaglutide lowered hsCRP roughly 30 percent in obesity trials, and FLOW reported similar inflammatory marker reductions.
- Direct GLP-1 receptor effects on renal tubular and vascular cells, although GLP-1 receptor expression in human kidney remains debated.
- Weight loss and improved cardiometabolic profile, which contribute but do not appear to fully explain the result.
For now, the honest framing is that FLOW established a kidney benefit at the outcomes level, while the mechanistic decomposition is ongoing in substudies.
Where FLOW sits in the broader CKD trial map
Three drug classes have produced randomised Phase 3 evidence for slowing diabetic kidney disease progression in patients on background RAAS blockade.
| Drug class | Pivotal Phase 3 | Population | Primary outcome reduction |
|---|---|---|---|
| SGLT2 inhibitor | DAPA-CKD (dapagliflozin) | CKD with or without T2D | 39% (HR 0.61) |
| SGLT2 inhibitor | EMPA-KIDNEY (empagliflozin) | Broad CKD with or without T2D | 28% (HR 0.72) |
| ns-MRA | FIDELIO-DKD (finerenone) | T2D with CKD | 18% (HR 0.82) |
| GLP-1 receptor agonist | FLOW (semaglutide) | T2D with CKD | 24% (HR 0.76) |
Note: Direct cross-trial comparison is unsafe. DAPA-CKD enrolled patients with and without diabetes, EMPA-KIDNEY enrolled at lower albuminuria thresholds, FIDELIO-DKD enrolled higher-albuminuria T2D, and FLOW enrolled at the most advanced eGFR thresholds. Each primary outcome composite differs slightly. The point of the table is to show that all four classes produced statistically significant reductions in the major kidney outcome relevant to their population.
What FLOW adds is the first dedicated Phase 3 evidence that a GLP-1 receptor agonist can do for diabetic kidney disease something analogous to what SGLT2s and finerenone do, with the added benefit of MACE and mortality reductions. The four classes appear to act on different parts of the disease pathway, which is why guidelines have started treating them as additive rather than competing.
Safety in FLOW: not the obesity-dose profile
Most of the public safety conversation around semaglutide draws on the 2.4 mg obesity dose trials. FLOW used 1.0 mg, the type 2 diabetes dose. That distinction matters when reading the FLOW safety table.
Serious adverse events were actually lower in the semaglutide group than placebo (49.6% vs 53.8%), consistent with the cardiovascular and kidney benefits reducing serious clinical events overall. Permanent discontinuation for adverse events was higher on semaglutide (13.2% vs 11.9%), with gastrointestinal events as the main driver, consistent with the known class profile.
Prespecified adverse events of special interest at or above 5%:
| Event | Semaglutide | Placebo |
|---|---|---|
| Diabetic retinopathy | 22.8% | 22.5% |
| COVID-19 related | 20.3% | 22.9% |
| Serious cardiovascular disorder | 15.4% | 18.1% |
| Heart failure | 7.5% | 9.9% |
| Acute kidney failure | 9.7% | 10.3% |
| Malignant tumor | 6.8% | 5.9% |
| Serious GI disorder | 5.4% | 5.3% |
The diabetic retinopathy signal that has shadowed semaglutide since SUSTAIN-6 did not separate from placebo in FLOW. Acute kidney failure was numerically lower on semaglutide, which mirrors the eGFR slope finding. The small numerical excess of malignancy is consistent with chance and with prior class trials, not a confirmed signal.
Warning: FLOW does not address pancreatitis, medullary thyroid cancer, or gallbladder disease at the granularity needed to update class-level labeling. Those signals remain at their pre-FLOW magnitudes. The semaglutide prescribing information continues to apply.
What FLOW does not say
A few framings of FLOW have been overstated. Worth keeping straight:
- FLOW does not establish semaglutide as a CKD drug in patients without type 2 diabetes. The closest analogous data is a prespecified analysis of the SELECT trial in obesity with established cardiovascular disease, where semaglutide reduced a five-component kidney composite by 22 percent (Colhoun et al., Nat Med 2024, PMID 38796653). That signal is supportive, not equivalent to FLOW.
- FLOW does not establish that other GLP-1 receptor agonists (dulaglutide, liraglutide, tirzepatide, retatrutide) confer the same kidney benefit. Each will require its own dedicated trial. A tirzepatide CKD trial has been discussed publicly but no Phase 3 readout exists yet.
- FLOW used 1.0 mg weekly. The kidney benefit at 2.4 mg, the obesity dose, was not tested in FLOW, although it would be reasonable to expect a similar or larger effect on mechanistic grounds.
- FLOW did not study compounded semaglutide. Compounded product quality and dosing accuracy fall outside the trial. If you are researching compounded semaglutide, the FDA 503A peptide compounding review covers the regulatory state.
How FLOW fits the broader GLP-1 indication map
The pattern across 2024-2026 GLP-1 indication trials has been mixed but informative.
| Indication | Pivotal trial | Result |
|---|---|---|
| Obesity | STEP, SURMOUNT | Established |
| Type 2 diabetes | SUSTAIN, SURPASS | Established |
| Cardiovascular (with established disease) | SELECT (semaglutide) | Positive |
| Heart failure (HFpEF, obesity-related) | STEP-HFpEF, SUMMIT (tirzepatide) | Positive |
| Sleep apnea | SURMOUNT-OSA (tirzepatide) | Positive |
| MASH | ESSENCE (semaglutide) | Positive |
| Chronic kidney disease (T2D) | FLOW (semaglutide) | Positive |
| Parkinson's | LIXIPARK, Exenatide-PD3 | Mixed (Phase 2 positive, Phase 3 negative) |
| Alzheimer's | EVOKE, EVOKE+ | Negative |
GLP-1 agonism continues to look strongest where cardiometabolic disease and the obesity-driven inflammation axis are the dominant drivers. CKD in T2D sits squarely in that lane, which is consistent with the FLOW result being clean and consistent across subgroups.
For broader context on where else this class has held up, see the ESSENCE Phase 3 MASH readout, the tirzepatide HFpEF SUMMIT trial, and the orforglipron oral Phase 3 review. For where it has not held up, the GLP-1 Alzheimer's evidence review and the Parkinson's negative Phase 3 results are the contrasting cases.
Practical implications for researchers and clinicians
FLOW did not change semaglutide's label on the day it was published. As of mid-2026, semaglutide remains FDA approved for type 2 diabetes (Ozempic and Rybelsus) and chronic weight management (Wegovy). The CKD outcomes data has been incorporated into the prescribing information and KDIGO guidelines but is not a standalone indication.
For practitioners managing T2D with CKD on background RAAS blockade and an SGLT2 inhibitor, FLOW shifts the calculus toward adding semaglutide for kidney and cardiovascular risk reduction, separately from glycemic control or weight management. This is the same pattern that emerged with SGLT2 inhibitors after DAPA-CKD and EMPA-KIDNEY: an outcomes trial that becomes the rationale for prescribing in a population the drug was not originally developed to treat.
For researchers, FLOW closes one question (does semaglutide help T2D CKD outcomes) and opens several:
- Does the benefit extend to nondiabetic CKD with obesity? Partial evidence in SELECT, not yet confirmed in a dedicated trial.
- Does tirzepatide produce a similar or larger effect? Plausible mechanistically, untested.
- Does the higher 2.4 mg obesity dose produce a larger kidney benefit, or does benefit plateau at the 1.0 mg dose? Unanswered.
- How long does the benefit persist beyond 3.4 years? FLOW follow-up will not address this; a dedicated extension study would be needed.
For researchers sourcing pharmacy-grade semaglutide for research, Ascension Peptides carries injectable semaglutide with code ENHANCED for 50% off. The GLP-1 muscle loss and lean mass preservation review and the stopping-GLP-1 weight regain literature cover adjacent questions for anyone designing protocols around this class.
Honest reading
FLOW is a clean Phase 3 with a positive primary, every prespecified secondary moving in the same direction, no meaningful heterogeneity by SGLT2 status or CKD severity, and a safety profile consistent with the established 1.0 mg semaglutide profile. The trial was stopped early because the data monitoring committee judged that continuing to randomise patients to placebo could no longer be justified given the size of the kidney signal. That is the strongest internal signal of confidence a Phase 3 trial can produce.
The trial does not transform GLP-1 receptor agonists into universal nephroprotective agents. It adds them, specifically semaglutide, to the diabetic kidney disease toolkit alongside SGLT2 inhibitors and finerenone. The trio is now the most evidence-backed combination for slowing CKD progression in T2D, and the FLOW SGLT2 subgroup analysis is what makes that combination claim defensible.
The Parkinson's and Alzheimer's negative readouts of 2026 narrowed the GLP-1 hypothesis. FLOW shows the cardiometabolic and renal core of the class is durable. Those two patterns are not in tension; they describe a drug class that does what it does (improve cardiometabolic disease) very well, and does not extend into territory where the mechanism does not apply.
References
- Perkovic V, et al. Effects of Semaglutide on Chronic Kidney Disease in Patients with Type 2 Diabetes. N Engl J Med. 2024;391(2):109-121. PMID 38785209
- Mann JFE, et al. Effects of semaglutide with and without concomitant SGLT2 inhibitor use in participants with type 2 diabetes and chronic kidney disease in the FLOW trial. Nat Med. 2024;30(10):2849-2856. PMID 38914124
- Pratley RE, et al. Effects of Semaglutide on Heart Failure Outcomes in Diabetes and Chronic Kidney Disease in the FLOW Trial. J Am Coll Cardiol. 2024;84(17):1615-1628. PMID 39217553
- Colhoun HM, et al. Long-term kidney outcomes of semaglutide in obesity and cardiovascular disease in the SELECT trial. Nat Med. 2024;30(7):2058-2066. PMID 38796653
- Rossing P, et al. The rationale, design and baseline data of FLOW, a kidney outcomes trial with once-weekly semaglutide in people with type 2 diabetes and chronic kidney disease. Nephrol Dial Transplant. 2023;38(9):2041-2051. PMID 36651820
- Mahaffey KW, et al. Cardiovascular outcomes with semaglutide by severity of chronic kidney disease in type 2 diabetes: the FLOW trial. Eur Heart J. 2025;46(12):1096-1108. PMID 39211948
- Tuttle KR, et al. Kidney and Survival Outcomes with Semaglutide by CKD Severity in the FLOW Trial. 2026. PMID 41706532
This article is for educational and research purposes only. None of the content above constitutes medical advice. Semaglutide is FDA approved as Ozempic for type 2 diabetes, as Wegovy for chronic weight management, and as Rybelsus for type 2 diabetes. It is not separately approved as a CKD therapy. Decisions about diabetic kidney disease care belong with the patient and their treating nephrologist or endocrinologist.