At a glance
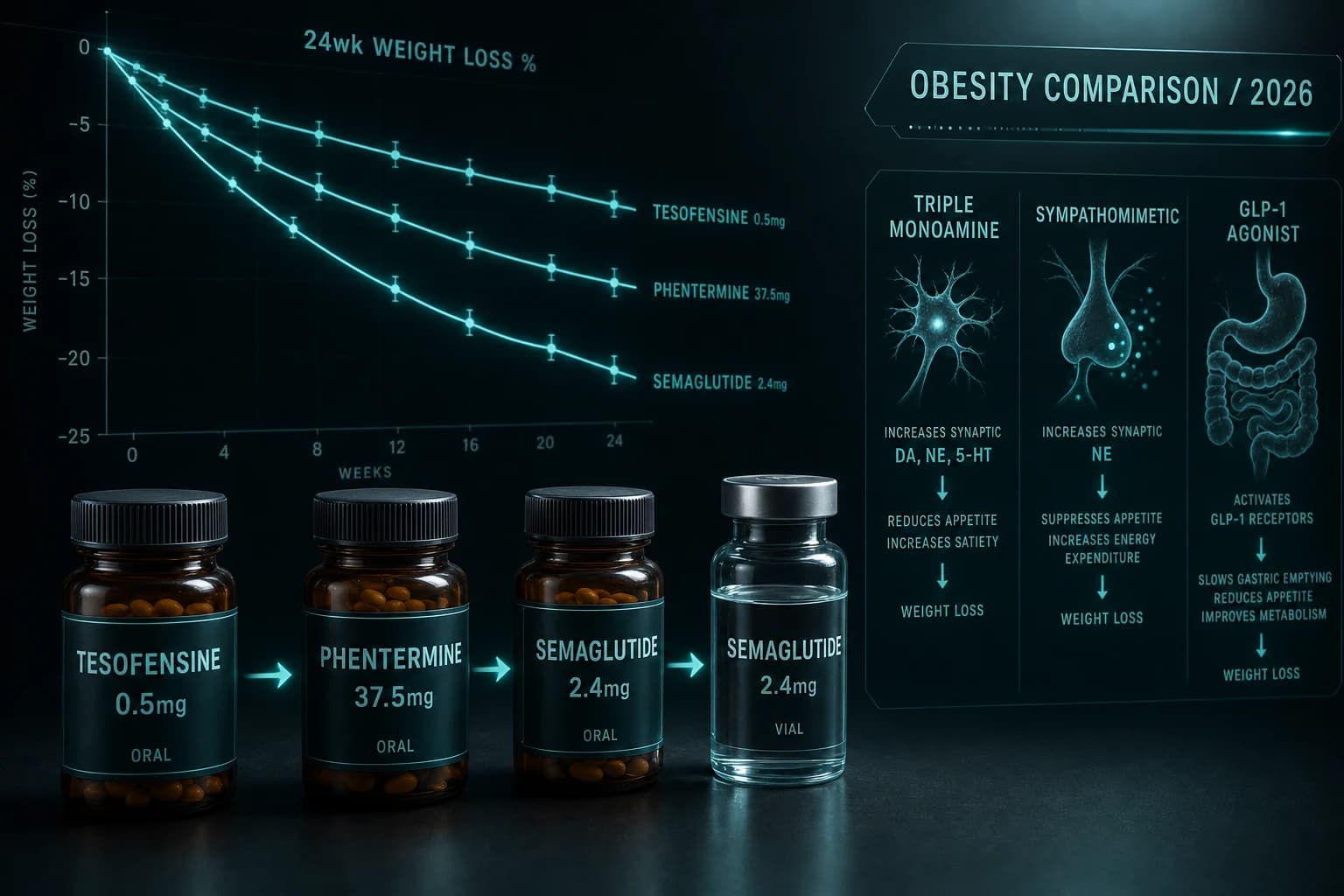
- Three mechanism categories: triple monoamine reuptake inhibition (tesofensine), sympathomimetic (phentermine), GLP-1 receptor agonism (semaglutide)
- Best published efficacy: semaglutide 2.4 mg at 14.9% at 68 wk (STEP 1); tesofensine 0.5 mg at 9.2% at 24 wk (Phase 2); phentermine 37.5 mg at 5-7% short-term
- Phentermine is FDA-approved for short-term obesity treatment (up to 12 weeks); semaglutide is approved for chronic weight management; tesofensine is research-only
- Phentermine has decades of established prescribing history and is the cheapest option ($10-40/month) but with lowest efficacy and short-term-only label
- For chronic weight management, semaglutide is the established choice; tesofensine offers similar Phase 2 efficacy with no Phase 3 confirmation
When someone weighs the GLP-1 class against older weight loss drugs, three compounds anchor the comparison: tesofensine (the research-grade triple monoamine reuptake inhibitor that produced 9.2% weight loss in Phase 2), phentermine (the decades-old sympathomimetic approved for short-term obesity treatment), and semaglutide (the GLP-1 receptor agonist that established the modern weight loss class). The three compounds work through entirely different mechanisms, have very different efficacy profiles, and serve different clinical situations.
This article covers the mechanism of each compound, the head-to-head efficacy data, the side effect profiles that differentiate them, and the practical decision framework for choosing between them in 2026 weight management research and clinical practice.
Three different mechanisms
| Compound | Class | Mechanism | Route | Status |
|---|---|---|---|---|
| Tesofensine | Triple monoamine reuptake inhibitor | Blocks reuptake of serotonin, norepinephrine, dopamine | Oral, once daily | Research-grade only |
| Phentermine | Sympathomimetic amine | Stimulates norepinephrine release | Oral, once daily | FDA approved (short-term obesity) |
| Semaglutide | GLP-1 receptor agonist | Activates GLP-1 receptors (satiety + slowed gastric emptying) | Injectable weekly or oral daily | FDA approved (chronic weight management) |
Tesofensine is the newest mechanism of the three. The triple monoamine reuptake inhibition profile is similar to bupropion (which has antidepressant indication) but with stronger dopamine reuptake inhibition. The mechanism affects appetite, energy expenditure, and reward signaling. Tesofensine was originally developed for Parkinson's and Alzheimer's disease, with weight loss noted as a side effect that prompted obesity development.
Phentermine is the oldest of the three. Approved in 1959 for short-term obesity treatment, phentermine is a sympathomimetic amine that stimulates norepinephrine release, producing appetite suppression and modest energy expenditure increase. The mechanism is similar to amphetamine but with reduced abuse potential, and phentermine is Schedule IV under federal scheduling.
Semaglutide is the modern mechanism standard. GLP-1 receptor agonism produces satiety through hindbrain circuits and slows gastric emptying, both contributing to reduced caloric intake. The mechanism is well-characterized and validated through extensive clinical trial programs.
For the broader GLP-1 dosing landscape including semaglutide, tirzepatide, and others, see the GLP-1 dosing comparison 2026.
Head-to-head efficacy
The published efficacy data:
| Compound | Trial | Dose | Duration | Mean weight loss | Reference |
|---|---|---|---|---|---|
| Semaglutide 2.4 mg | STEP 1 | 2.4 mg weekly | 68 wk | -14.9% | Wilding 2021 |
| Semaglutide 7.2 mg | STEP UP | 7.2 mg weekly | 72 wk | -20.7% | Wegovy HD approval, 2026 |
| Tesofensine 0.5 mg | Phase 2 | 0.5 mg daily | 24 wk | -9.2 ppt placebo-adjusted | Astrup 2008 |
| Tesofensine 1.0 mg | Phase 2 | 1.0 mg daily | 24 wk | -10.6 ppt placebo-adjusted | Astrup 2008 |
| Phentermine 37.5 mg | Various | 37.5 mg daily | 12 wk | -5 to -7% | Multiple trials |
| Phentermine + topiramate (Qsymia) | CONQUER | Combo | 56 wk | -9.8% | Gadde 2011 |
The efficacy ranking at matched durations:
- Top: Semaglutide 7.2 mg (20.7% at 72 wk) > Semaglutide 2.4 mg (14.9% at 68 wk)
- Middle: Tesofensine 0.5 mg (10-11% at 24 wk) > Phentermine + topiramate (9.8% at 56 wk)
- Lower: Phentermine alone (5-7% at 12 wk maximum FDA-approved duration)
Semaglutide produces the largest weight loss at the longer durations the drug has been studied. Tesofensine at 24 weeks produces approximately the same total weight loss as semaglutide at 24 weeks, but tesofensine has no published 68-week data to extend the comparison.
Phentermine produces modest weight loss in 12-week trials, which is the maximum FDA-approved duration. Off-label longer phentermine use is common but not directly supported by trial data and carries cumulative cardiovascular concerns.
Bottom line: Semaglutide is the clear efficacy leader at long durations. Tesofensine matches semaglutide at shorter durations but has no Phase 3 long-duration data. Phentermine produces modest short-term weight loss and is appropriate for short-term clinical situations rather than chronic weight management.
Side effect profiles compared
The class-specific side effects differ substantially:
Tesofensine. Triple monoamine reuptake inhibition produces:
- Dry mouth (45% at 0.5 mg vs 20% placebo)
- Nausea (24% at 0.5 mg vs 11% placebo)
- Constipation
- Insomnia (especially at higher doses or evening dosing)
- Heart rate increase (+7.4 bpm at 0.5 mg)
- Mood and anxiety changes (more pronounced at 1.0 mg)
Phentermine. Sympathomimetic class:
- Dry mouth
- Insomnia (the primary dose-limiting effect)
- Heart rate increase (typically more pronounced than tesofensine)
- Blood pressure elevation
- Anxiety and restlessness
- Constipation
- Schedule IV controlled substance (abuse potential, though limited)
Semaglutide. GLP-1 class:
- Nausea (most common, peaks during titration)
- Vomiting
- Diarrhea and constipation
- Decreased appetite (this is the mechanism, not a side effect, but it affects QoL)
- Injection-site reactions
- Less cardiovascular profile concern; some patients develop tachycardia
For semaglutide-specific dosing and side effect details, see the Wegovy HD 7.2 mg STEP UP trial guide. For tesofensine-specific dosing, see the Tesofensine dosage guide 2026.
The practical decision framework
For 2026 clinical decision-making, the choice between these three depends on several factors:
Choose semaglutide if:
- Chronic weight management is the goal (label-supported)
- Patient can tolerate weekly injection (or oral Rybelsus for those who cannot)
- Insurance covers semaglutide or patient can afford branded/compounded
- Patient prefers GLP-1 mechanism (proven, well-studied)
Choose phentermine if:
- Short-term obesity treatment is the goal (FDA approved up to 12 weeks)
- Cost is the primary constraint ($10-40/month)
- Patient prefers oral therapy over injection
- No cardiovascular contraindications
Choose tesofensine if:
- Research context where the mechanism is the question
- Patient cannot use GLP-1 or phentermine for specific reasons
- Comfortable with research-grade-only regulatory status
- Patient and clinician accept the absence of Phase 3 data
The honest reality: for chronic weight management in 2026, semaglutide is the established choice. Tesofensine and phentermine occupy niche positions where specific situations favor their mechanisms, but neither displaces semaglutide as the default chronic weight management option.
Cost and access
| Compound | Cost range | Insurance reality |
|---|---|---|
| Phentermine | $10-40/month (generic) | Often covered; short-term only |
| Tesofensine (research-grade) | $50-100/month equivalent | Not covered (research-grade) |
| Semaglutide branded (Wegovy/Ozempic) | $500-1,400/month cash | Variable coverage |
| Semaglutide compounded | $150-400/month | Not covered; narrowing access |
| Semaglutide research-grade | $30-80 per 5 mg vial | Not covered |
The cost gap between phentermine (cheapest) and semaglutide branded (most expensive) is 50-100x. The compounded semaglutide and research-grade tesofensine occupy middle pricing tiers. For coverage of generic semaglutide timing, see the generic semaglutide patent expiry timeline 2026.
Pairing with other research peptides
These three compounds are sometimes combined with other research approaches:
Tesofensine + recovery peptides. Some research stacks combine tesofensine with BPC-157, TB-500, or GHK-Cu for body composition research. The combination has not been formally trial-tested.
Phentermine + topiramate (Qsymia). This is an FDA-approved combination product where the topiramate component adds additional weight loss benefit beyond phentermine alone. The CONQUER trial showed 9.8% weight loss at 56 weeks (Gadde et al., 2011).
Semaglutide + recovery peptides. Common in athletic and post-bariatric research. The peptide component addresses tissue repair while semaglutide drives weight loss. See the GLP-1 muscle loss research for the lean mass preservation context.
What is changing in 2026
Three factors are reshaping this comparison through 2026:
1. Wegovy HD 7.2 mg approval (March 2026). Wegovy HD pushes semaglutide's top dose from 2.4 mg (14.9% weight loss) to 7.2 mg (20.7% weight loss), widening the efficacy gap versus tesofensine and phentermine.
2. Tirzepatide and retatrutide pipeline. The newer GLP-1/GIP and triple-agonist compounds make even tesofensine's strong Phase 2 number look modest. Tirzepatide 15 mg produces 22.5% at 72 weeks; retatrutide 12 mg produces 24.2% at 48 weeks.
3. Generic semaglutide approaching (2032). The current branded pricing on semaglutide will face substantial pressure when generics arrive. This affects the cost-benefit math versus cheaper phentermine and may eliminate the price-driven case for non-GLP-1 alternatives.
For the broader 2026 obesity landscape, see the GLP-1 dosing comparison 2026 and the Wegovy HD 7.2 mg STEP UP trial guide.
FAQ
Which produces the most weight loss?
Semaglutide 7.2 mg (Wegovy HD) at 20.7% mean weight loss at 72 weeks. Semaglutide 2.4 mg at 14.9% at 68 weeks. Tesofensine 0.5 mg at 9-11% at 24 weeks (shorter duration). Phentermine alone at 5-7% at 12 weeks. The ranking at matched durations strongly favors semaglutide.
Is tesofensine better than semaglutide?
At 24 weeks, tesofensine 0.5 mg produces approximately the same total weight loss as semaglutide 2.4 mg at 24 weeks. Tesofensine has no published longer-duration data, while semaglutide has been extensively studied at 68-72 weeks. For chronic weight management decisions, semaglutide has the validated long-duration profile.
Why is phentermine limited to short-term use?
Phentermine is approved for short-term obesity treatment because: (1) tolerance develops with continued use (weight loss plateaus), (2) cardiovascular concerns increase with prolonged sympathomimetic exposure, and (3) the Schedule IV controlled-substance status discourages long-term continuous prescribing. Off-label long-term use exists but is not directly supported by trial data.
Can I combine these compounds?
Phentermine + topiramate is an FDA-approved combination (Qsymia). Other combinations are not formally tested. Combining tesofensine with semaglutide is not standard and combines overlapping appetite-suppression mechanisms that may cumulatively produce excessive side effects. Most patients on weight loss therapy use one primary compound rather than multiple.
Is phentermine safe long-term?
The cardiovascular concerns with long-term sympathomimetic use are well-documented. Sustained phentermine elevates heart rate and may elevate blood pressure, potentially contributing to cardiovascular events over time. Patients with pre-existing cardiovascular disease should not use phentermine. Phentermine is approved for short-term use, and continued use beyond approved duration is off-label.
Will generic tesofensine be available?
Tesofensine remains research-grade only as of May 2026. Phase 3 development was never completed; NeuroSearch restructured during the planned Phase 3 era. Unless a new sponsor advances the compound through Phase 3 and approval, no commercial generic tesofensine pathway exists.
What about Wegovy HD vs the others?
Wegovy HD (semaglutide 7.2 mg) at 20.7% weight loss at 72 weeks is meaningfully ahead of tesofensine and substantially ahead of phentermine. For patients who tolerate semaglutide at 2.4 mg and want more weight loss, the HD escalation is the validated pathway. See the Wegovy HD 7.2 mg STEP UP trial guide.
Further reading
- Tesofensine dosage guide 2026
- GLP-1 dosing comparison 2026
- Wegovy HD 7.2 mg STEP UP trial guide
- Oral semaglutide (Rybelsus) vs orforglipron guide
- Tirzepatide vs Semaglutide 2026 head-to-head
- Retatrutide vs Tirzepatide vs Semaglutide
- 5-Amino-1MQ NNMT inhibitor research review
- GLP-1 muscle loss lean mass preservation research
- Generic semaglutide patent expiry timeline 2026
- Best legit peptide vendors 2026
This article is for educational and informational purposes only. Phentermine is FDA-approved for short-term obesity treatment under a Schedule IV controlled-substance designation. Semaglutide is FDA-approved as Wegovy for chronic weight management and as Ozempic for type 2 diabetes. Tesofensine is sold under research-use disclosures and is not approved by the FDA. None of the content above constitutes medical advice. Patients should consult a qualified clinician for individual decisions about weight management therapy.