At a glance
- Yen 2024 (PMID 37331413, 467 propensity-matched pairs) found GLP-1 RAs lowered decompensation (aHR 0.70), hepatic encephalopathy (aHR 0.59), liver failure (aHR 0.54), and all-cause death (aHR 0.47) in compensated cirrhosis with T2D.
- Wang 2024 (PMID 38692395, 1.89M T2D patients, 5-year follow-up) found GLP-1 RAs reduced HCC incidence and hepatic decompensation versus non-GLP-1 comparators.
- UCLA cohort Chow et al. 2024 (PMID 37639288): 23 post-transplant patients on semaglutide up to 2 mg/week lost about 5% body weight over the follow-up window with 65% reporting no side effects.
- Grancini 2025 (PMID 40496570, n=68 Italian LT recipients): 18 months of GLP-1 added to metformin or insulin cut HbA1c, weight, BMI, waist, and LDL with no graft dysfunction reported.
- Sarno 2026 (PMID 41884702, TriNetX, 546 matched pairs): post-transplant GLP-1 use was not associated with worse mortality, hospitalization, or graft outcomes versus matched non-users.
- There is still no completed Phase 3 trial of any GLP-1 RA in cirrhosis or post-transplant populations. NCT05424003 (semaglutide for post-LT weight gain) is the closest active RCT.
Why cirrhosis and transplant got pushed aside in the GLP-1 story
Almost every Phase 3 GLP-1 trial that built this class excluded the patients who arguably need GLP-1 mechanisms the most. STEP, SURMOUNT, SELECT, SUSTAIN, REWIND, and ESSENCE all enrolled either non-cirrhotic obesity, type 2 diabetes with intact liver synthetic function, or F2 to F3 fibrosis without portal hypertension. People with decompensated cirrhosis, on the transplant list, or post-transplant on tacrolimus were never the trial population. The result is a real-world gap: hepatologists started using semaglutide and tirzepatide in cirrhotic patients with type 2 diabetes years before the labels caught up, and the evidence base is mostly cohort studies and single-center series.
The 2024 to 2026 evidence has finally accumulated enough that the question is no longer "is this safe at all" but "where does it fit, and what does the magnitude of effect actually look like." Three signals are now reasonably consistent across independent datasets. GLP-1 RAs reduce decompensation in compensated cirrhosis with T2D. They produce real weight loss in liver transplant recipients with manageable side effects. And so far, no large cohort has surfaced a graft survival or rejection signal that would force a stop on the existing use pattern.
Bottom line: Across propensity-matched cohorts (Yen 2024, Wang 2024, Sarno 2026), GLP-1 receptor agonists in cirrhosis with diabetes are associated with lower decompensation, hepatic encephalopathy, and mortality. Post-transplant data in single-center and TriNetX cohorts shows weight loss and glycemic improvement without an excess of rejection or graft dysfunction. None of this is randomized trial data yet. NCT05424003 (semaglutide for post-LT weight gain) is the closest active RCT and has not reported.
The two clinical questions sitting underneath this evidence
Hepatology has two distinct GLP-1 questions running in parallel. Both deserve a separate read.
| Question | Population | Best available evidence |
|---|---|---|
| "Should we use a GLP-1 in compensated cirrhosis with T2D?" | Child-Pugh A, MASH or alcohol-related, type 2 diabetes | Cohort studies (Yen 2024, Wang 2024) plus the ESSENCE Phase 3 MASH readout in non-cirrhotic F2-F3 |
| "Can we use a GLP-1 after liver transplant?" | Post-LT recipients with NODAT, recurrent MASH, or weight regain | Single-center series (Chow 2024 UCLA, Grancini 2025 Milan), retrospective propensity-matched cohort (Sarno 2026 TriNetX) |
The decompensated cirrhosis question (Child-Pugh B or C, refractory ascites, recurrent HE, hepatorenal syndrome) sits outside both of those rows. There is essentially no usable evidence in advanced decompensation, and the existing case literature is dominated by one cautionary report of rapid weight loss precipitating decompensation in a MASH-cirrhosis patient (Boyer-Diaz et al., J Hepatol 2024, PMID 38186682). That report is a single case, but it is the cleanest published flag that decompensated cirrhosis is not the population this evidence base supports.
Compensated cirrhosis with T2D: what the propensity-matched cohorts show
The cleanest dataset on compensated cirrhosis with type 2 diabetes is the Taiwan National Health Insurance Database cohort published by Yen and colleagues in Clinical Gastroenterology and Hepatology in 2024 (Yen et al., CGH 2024, PMID 37331413). The investigators used propensity-score matching to assemble 467 pairs of GLP-1 RA users and non-users with biopsy-confirmed or clinically diagnosed compensated cirrhosis and T2D, drawn from a national insurance dataset between 2008 and 2019. Mean follow-up was about 4 years.
Effect sizes across endpoints were directionally consistent and large. Mortality rates were 27.46 per 1,000 person-years on GLP-1 RAs versus 55.90 per 1,000 person-years off, an adjusted hazard ratio of 0.47. Decompensated cirrhosis came in at aHR 0.70. Hepatic encephalopathy was 0.59. Liver failure was 0.54. Cardiovascular events were 0.60. Longer cumulative GLP-1 RA exposure produced a larger effect. That dose-response pattern across all five endpoints is the main reason this cohort is taken seriously and not dismissed as channeling bias.
A companion read on a larger US dataset comes from Wang and colleagues in Gastroenterology, who ran a retrospective cohort across nearly 1.89 million adults with type 2 diabetes and no prior HCC (Wang et al., Gastroenterology 2024, PMID 38692395). Patients prescribed GLP-1 RAs were compared against those on insulin, metformin, SGLT2 inhibitors, DPP-4 inhibitors, sulfonylureas, and thiazolidinediones during a 5-year follow-up window. Incident HCC and hepatic decompensation were both significantly lower on GLP-1 RAs versus most comparators, with the largest gap against insulin and sulfonylureas. The cohort was not restricted to cirrhosis at baseline, so the absolute hepatic event rates were lower than in Yen, but the comparator structure mirrors what a clinician actually faces when picking a second-line agent.
Hwang and colleagues replicated the pattern at a smaller scale in the All of Us Research Program: GLP-1 RA use was associated with a reduced risk of hepatic decompensation versus DPP-4 inhibitors (HR 0.67, 95% CI 0.47-0.95) in a propensity-matched analysis of patients with cirrhosis and diabetes. Three cohorts using different data sources, different comparators, and different inclusion criteria converging on the same direction is what hepatology has, short of a randomized trial.
| Cohort | Population | Comparator | Decompensation HR (95% CI) | Mortality HR (95% CI) |
|---|---|---|---|---|
| Yen 2024 (Taiwan NHIRD) | n=934, compensated cirrhosis + T2D | Non-GLP-1 antidiabetic | 0.70 (0.49-0.99) | 0.47 (0.36-0.61) |
| Wang 2024 (US claims) | n=1.89M, T2D (not restricted to cirrhosis) | Other antidiabetics | Lower across multiple comparators | Lower across multiple comparators |
| Hwang 2026 (All of Us) | Cirrhosis + T2D subgroup | DPP-4 inhibitors | 0.67 (0.47-0.95) | Not the primary endpoint |
| Kanwal 2023 (TriNetX, dual therapy) | Cirrhotic T2D, metformin plus GLP-1 vs metformin alone (PMID 37664227) | Metformin monotherapy | 0.65 (0.46-0.93) | Lower |
The 2026 GRADE-style synthesis of these and adjacent cohorts is the systematic review by Pasta and colleagues in the European Journal of Clinical Investigation, which pooled the cohort evidence on HCC and decompensation. The pooled signal favored GLP-1 RAs on both endpoints, with moderate certainty given that all contributing studies are observational. No randomized trial in cirrhosis has reported as of June 2026.
Note: None of the cohort effects above proves causality. Confounding by indication is the standard concern: clinicians who prescribe GLP-1 RAs in cirrhosis may already be selecting healthier, more adherent, more metabolically active patients. The dose-response gradient in Yen 2024 is the strongest argument against pure selection, but it does not eliminate it. The next decisive evidence will come from a controlled trial. Until then, treat the magnitude estimates as plausible upper bounds, not point estimates.
Where the ESSENCE Phase 3 readout fits
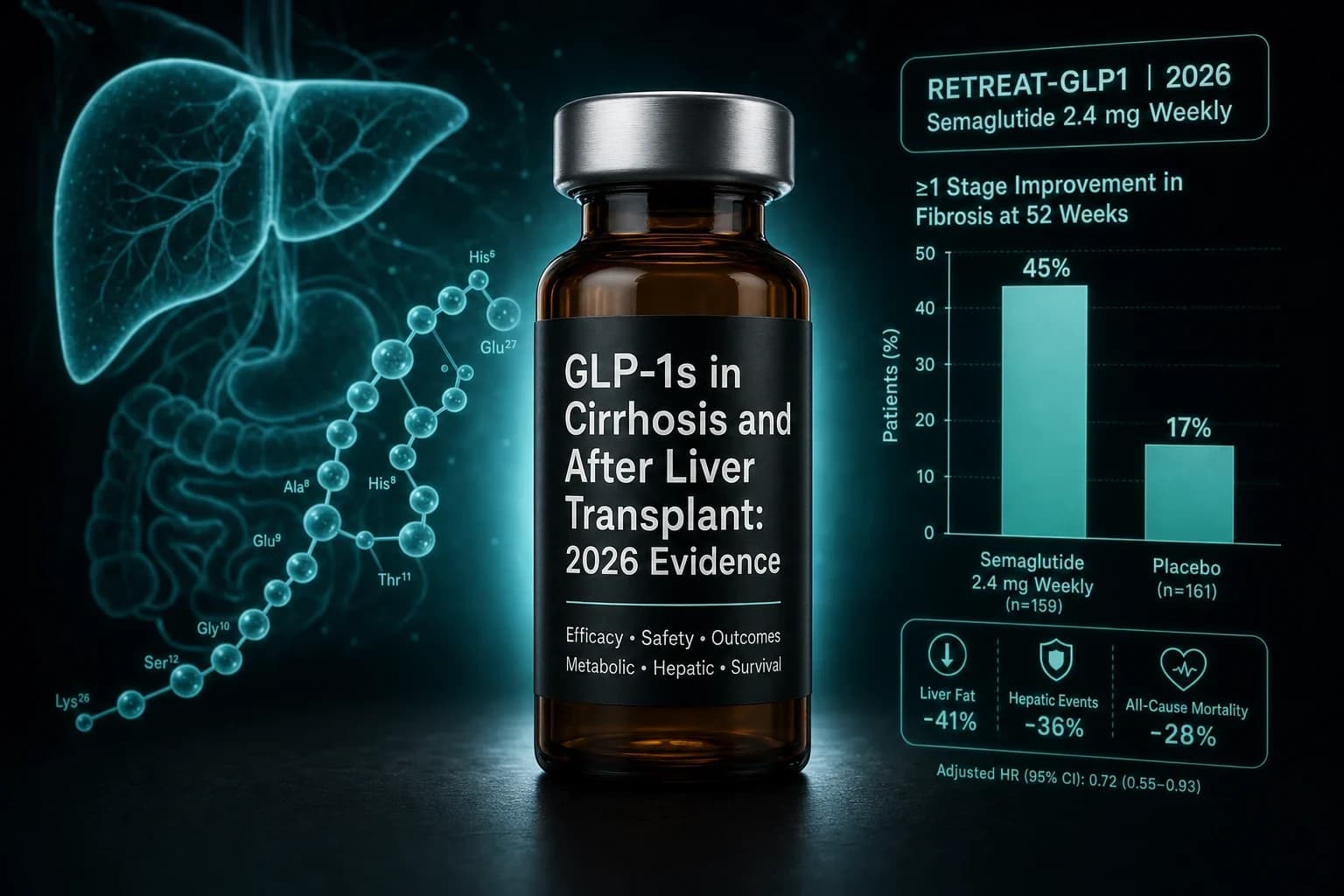
The largest randomized read in advanced liver disease for any GLP-1 RA is the ESSENCE Phase 3 trial of semaglutide 2.4 mg in MASH with F2 to F3 fibrosis (Newsome et al., NEJM 2025). The full breakdown of that trial is covered in our semaglutide MASH ESSENCE Phase 3 evidence review. The single sentence that matters here is that ESSENCE excluded F4 cirrhosis. The signals on MASH resolution and fibrosis improvement at 72 weeks therefore do not directly read into the compensated cirrhosis question. They support the underlying mechanistic case (weight loss and metabolic improvement reduce hepatic inflammation and fibrosis trajectory) but they do not establish that semaglutide reverses cirrhosis or prevents decompensation in patients already at F4.
An identical caveat applies to the tirzepatide MASH SYNERGY-NASH Phase 2 data and the pemvidutide IMPACT Phase 2b readout. Phase 2 and Phase 3 MASH programs excluded cirrhotics by design. Cohort data on cirrhosis is hypothesis-generating in a separate population the trials have not yet reached.
One active trial would actually close this loop: NCT05424003, a randomized, double-blinded, placebo-controlled trial of semaglutide for prevention of weight gain after liver transplantation. As of June 2026 it is enrolling but has not reported a primary endpoint. SYNCHRONIZE (survodutide MASH Phase 3) is the next adjacent Phase 3 with cirrhotic enrollment in a subset, with a topline read expected in late 2026.
Post-transplant: weight gain, NODAT, and recurrent MASH
The transplant population is its own clinical problem. About 30 to 40% of liver transplant candidates have type 2 diabetes at the time of transplant, and another 15 to 25% develop new-onset diabetes after transplantation (NODAT) within the first three years, driven by tacrolimus, steroids, and weight gain (review in the AASLD Liver Fellow Network curriculum). Weight regain is also the dominant medium-term complication of transplant for MASH-cirrhosis recipients, and recurrent steatohepatitis on the new graft is increasingly recognized in long-term cohorts. None of these problems have a clean pharmacologic answer, which is why GLP-1 RAs have been adopted by transplant hepatologists faster than the evidence base would normally justify.
First usable cohort on post-transplant semaglutide is the UCLA Pfleger Liver Institute series published by Chow and colleagues in Liver Transplantation in 2024 (Chow et al., Liver Transplant 2024, PMID 37639288). The investigators retrospectively identified 23 adult orthotopic liver transplant recipients prescribed semaglutide for at least 3 continuous months post-transplant. Mean age was 65, ethnically diverse, and most patients were on tacrolimus-based immunosuppression. Mean baseline weight was 92 kg and dropped to 87 kg at last follow-up (p=0.0024), a 5% mean weight loss. Nineteen of 23 patients lost weight. Side effects were the expected GLP-1 pattern: nausea 30%, vomiting 26%, early satiety 6%, diarrhea 2%, and 65% reported no adverse events at all.
Milan replicated the signal in the Grancini cohort published in Frontiers in Endocrinology in 2025 (Grancini et al., Front Endocrinol 2025, PMID 40496570). Sixty-eight LT recipients with post-transplant diabetes were started on subcutaneous semaglutide, subcutaneous dulaglutide, or oral semaglutide as an add-on to metformin or insulin and followed for 18 months. Fasting plasma glucose, HbA1c, weight, BMI, waist circumference, total cholesterol, and LDL cholesterol all dropped significantly. The investigators reported no graft dysfunction, no acute rejection episodes attributable to the GLP-1, and no clinically meaningful changes in tacrolimus trough levels.
Largest sample size to date is the Sarno propensity-matched TriNetX cohort published in 2026 (Sarno et al., 2026, PMID 41884702). The authors identified 546 liver transplant recipients prescribed semaglutide, dulaglutide, or liraglutide within one month post-transplant and matched them 1:1 to non-users on age, sex, ethnicity, cause of cirrhosis, immunosuppression regimen, and comorbidity burden. The comparator pool was over 37,000 non-users. Across all-cause mortality, cardiovascular events, renal events, respiratory events, and graft outcomes through follow-up, the GLP-1 arm did not show excess risk. The signal was directionally favorable on metabolic endpoints. This is the closest thing to a graft-safety read the field has, and the absence of a rejection or graft-loss signal across 546 paired patients is meaningful even though it is not randomized.
A single-center series by Imaeda and colleagues adds a propensity-matched comparison against insulin in 38 post-LT recipients (Imaeda et al. 2025, PMID 40128152). Weight, BMI, and HbA1c all improved on GLP-1 versus insulin; no graft rejection or unexpected tacrolimus dose adjustments were reported.
| Post-transplant cohort | n | Drug | Follow-up | Weight change | Safety signal |
|---|---|---|---|---|---|
| Chow 2024 (UCLA) | 23 | Semaglutide up to 2 mg/wk | At least 3 months | -5% mean (92 to 87 kg, p=0.0024) | 65% no side effects; nausea 30% |
| Grancini 2025 (Milan) | 68 | Semaglutide, dulaglutide, oral semaglutide | 18 months | Significant BMI and waist drop | No graft dysfunction; LDL and HbA1c improved |
| Imaeda 2025 (single center) | 38 | GLP-1 RA vs insulin (propensity-matched) | Variable | Favored GLP-1 | No rejection signal |
| Sarno 2026 (TriNetX, 546 pairs) | 1,092 | Semaglutide, dulaglutide, liraglutide | Through 2023 follow-up | Not the primary endpoint | No excess mortality, hospitalization, or graft loss |
Tip: The Chow, Grancini, Imaeda, and Sarno cohorts all use real-world post-LT prescribing patterns, which means dose titration was clinician-driven, not protocolized. The 2 mg semaglutide dose in Chow is consistent with the obesity-indication maximum but is on the upper end of what most transplant centers initiate. Most clinicians titrate over 12 to 16 weeks rather than the 8 weeks used in the obesity Phase 3 program, partly to limit nausea against a baseline of post-LT GI sensitivity.
Drug interactions: tacrolimus, mycophenolate, and the gastric-emptying question
The drug interaction concern that delayed adoption of GLP-1 RAs in transplant populations was straightforward: GLP-1s slow gastric emptying, and tacrolimus has a narrow therapeutic window and erratic GI absorption. The hypothetical was that a 2 to 4 hour delay in tacrolimus Tmax could produce subtherapeutic troughs, which in turn could allow rejection.
Available evidence on this hypothesis is mostly reassuring. In the Grancini 18-month cohort, no clinically meaningful tacrolimus trough changes were observed and no dose adjustments outside the normal post-transplant pattern were required. In the smaller liraglutide case series referenced in the post-transplant pharmacotherapy reviews, concomitant liraglutide and tacrolimus dosing did not produce trough changes that required adjustment. The mechanistic plausibility of an interaction is real, but the magnitude in clinical use appears small enough that standard tacrolimus trough monitoring catches it.
Two practical recommendations now appear consistently in the post-LT prescribing literature:
- Check the tacrolimus trough at 2 to 4 weeks after GLP-1 initiation and at each dose escalation. If a trough drift is detected, it is almost always upward, not downward, because GLP-1 weight loss reduces volume of distribution.
- Watch for the orlistat-style reduction-in-absorption pattern, which has been reported for a different obesity drug. About 50% of liver transplant recipients on orlistat required tacrolimus dose adjustment in older series; the comparable figure for GLP-1 RAs is much lower but the active monitoring is the same.
Mycophenolate, cyclosporine, and sirolimus interactions are smaller in magnitude than tacrolimus and have not surfaced as practical issues in the published cohorts. The post-LT pharmacology reviews flag mTOR-inhibitor and GLP-1 co-use as theoretically interesting (both have weight and metabolic effects) but there is no usable randomized evidence to inform that combination.
The decompensation case: where this evidence does not apply
The case report most often cited as the cautionary footnote in this literature is the J Hepatol 2024 description of a 60-year-old patient with NASH-related cirrhosis who developed rapid weight loss on semaglutide and then acutely decompensated with ascites and hepatic encephalopathy (PMID 38186682). The mechanism proposed was sarcopenia and protein catabolism in a patient with marginal hepatic reserve, where rapid weight loss removed the metabolic buffer that was keeping the cirrhosis compensated. Single case, no controlled comparison, and the underlying patient profile (advanced NASH-cirrhosis with marginal synthetic function) is one that should not have been started on a GLP-1 in the first place under most modern guidance.
Implication is not that cirrhotics cannot use GLP-1 RAs. It is that the GLP-1 cirrhosis evidence base is built on compensated Child-Pugh A patients with type 2 diabetes, and the magnitude of effect estimates do not transfer to Child-Pugh B and C disease without separate evidence. Three populations are still off-evidence:
- Child-Pugh C cirrhosis or MELD greater than 20.
- Active or refractory ascites.
- Recurrent overt hepatic encephalopathy.
For those populations, the case literature is too thin to support a generalizable recommendation, and the prudent default is to defer GLP-1 initiation until transplant or until decompensation resolves on standard hepatology management. Sarcopenia is the specific concern that hepatology has flagged across multiple reviews, and the GLP-1 muscle loss research summary applies with extra force in a population where loss of skeletal muscle is itself a decompensation trigger.
Warning: Rapid weight loss in advanced cirrhosis can precipitate decompensation through several distinct mechanisms: sarcopenia and protein catabolism reducing hepatic synthetic reserve, volume shifts altering portal pressure dynamics, and altered drug pharmacokinetics. The GLP-1 cirrhosis evidence base is in compensated Child-Pugh A patients. Extrapolation to Child-Pugh B or C is not supported by current data, and the Boyer-Diaz case report is the cleanest published example of how this can go wrong.
Drug choice within the class: where the data is and is not
Most of the cirrhosis and post-transplant evidence is on semaglutide and dulaglutide, with smaller series on liraglutide. Tirzepatide post-transplant data is much sparser; the published post-LT cohorts are dominated by semaglutide because the drug was available first. The tirzepatide kidney signal in the SURPASS-CVOT exploratory analysis (Nicholls et al., NEJM 2025) is encouraging on adjacent organ endpoints but does not directly speak to the liver or graft question. The SURPASS-CVOT tirzepatide vs dulaglutide evidence review covers the cardiovascular and renal subgroup data in detail.
Retatrutide, the GLP-1/GIP/glucagon triple agonist, has no published cirrhosis or transplant cohort. The Phase 2 obesity readout (Jastreboff et al., NEJM 2023, PMID 37356073) excluded cirrhosis, and the TRIUMPH-1 Phase 3 published in 2026 maintained that exclusion. For the clinical Phase 3 retatrutide context, the retatrutide TRIUMPH-1 Phase 3 review is the cleanest current read.
The dual GLP-1/glucagon program (survodutide, mazdutide, pemvidutide) deserves separate attention because glucagon agonism has independent hepatic effects on lipid handling and could be particularly relevant in MASH-cirrhosis. The dedicated readouts so far are in F2 to F3 fibrosis without cirrhosis. SYNCHRONIZE (survodutide MASH Phase 3) is the only Phase 3 with cirrhotic enrollment in a subset, with a topline read expected in late 2026.
| Drug class within GLP-1 | Cirrhosis cohort data | Post-transplant cohort data | Phase 3 cirrhosis trial |
|---|---|---|---|
| Semaglutide (GLP-1 mono) | Yen 2024, Wang 2024, Hwang 2026 | Chow 2024 UCLA, Grancini 2025, Sarno 2026 | ESSENCE excluded F4; NCT05424003 active post-LT |
| Dulaglutide (GLP-1 mono) | Yen 2024 (subset), Grancini 2025 | Grancini 2025, Sarno 2026 | None active |
| Liraglutide (GLP-1 mono) | Small case series | Small case series, Sarno 2026 | None active |
| Tirzepatide (GLP-1/GIP) | No published cirrhosis cohort | No published post-LT cohort | SURPASS-CVOT included CKD subgroup; no liver-specific Phase 3 |
| Survodutide (GLP-1/glucagon) | None | None | SYNCHRONIZE Phase 3 enrolling, cirrhotic subset, 2026 readout |
| Pemvidutide (GLP-1/glucagon) | None | None | IMPACT Phase 2b reported; Phase 3 in MASH planned |
| Retatrutide (GLP-1/GIP/glucagon) | None | None | TRIUMPH excluded cirrhosis |
Practical framework for 2026
The current evidence supports a tiered approach that mirrors what most transplant hepatology groups are doing in practice. The framework below summarizes the consensus pattern across the AASLD Liver Fellow Network curriculum, the post-transplant pharmacotherapy review literature, and the published cohort studies.
-
Compensated Child-Pugh A cirrhosis with type 2 diabetes. GLP-1 RA is a reasonable second-line agent after metformin in patients without contraindications. The Yen 2024 and Wang 2024 effect sizes are large enough that the metabolic benefit outweighs the conservatively framed sarcopenia risk in this population. Standard titration over 12 to 16 weeks limits nausea and rapid weight loss.
-
Compensated Child-Pugh A cirrhosis without diabetes. Less data. The evidence base is dominated by T2D cohorts. Use is reasonable in the MASH-cirrhosis subset where the ESSENCE evidence in F2-F3 and the tirzepatide SYNERGY-NASH Phase 2 data provide the mechanistic backstop. Outside MASH, the case is weaker.
-
Decompensated cirrhosis (Child-Pugh B or C). Off-evidence. Defer until transplant or until decompensation resolves. The Boyer-Diaz case report and the sarcopenia mechanism make this the correct conservative default.
-
On the transplant waitlist. Mixed practice. Some centers use GLP-1 RAs to bring BMI under the listing threshold in MASH-cirrhotic candidates with compensated disease. The DDW 2026 cirrhosis data on GLP-1 use reducing transplant need is hypothesis-generating but not yet peer-reviewed at the level of a published cohort.
-
Post-transplant with NODAT or weight regain. Evidence-supported, with standard tacrolimus monitoring. Semaglutide is the agent with the largest dataset (Chow, Grancini, Sarno). Initiation 6 months or more post-transplant is the modal practice in published cohorts.
-
Post-transplant with recurrent MASH on the graft. Reasonable on mechanism and on the early Grancini data, but the formal Phase 3 evidence is not yet published. NCT05424003 will be the most decisive read when it reports.
Bottom line: The 2026 evidence supports GLP-1 RAs in compensated cirrhosis with type 2 diabetes and post-transplant for NODAT or weight regain. It does not support GLP-1 use in decompensated cirrhosis. Post-transplant tacrolimus trough monitoring catches the only documented drug interaction. Phase 3 trial data in cirrhosis populations is still pending across the entire class.
Sourcing for researchers tracking the hepatology endpoint set
Researchers tracking the GLP-1 hepatology endpoint set typically follow semaglutide, tirzepatide, and retatrutide for the dominant Phase 3 programs. For the injectable research compounds in this class with lot-level COA availability, Ascension Peptides covers the catalog with code ENHANCED for 50 percent off. For oral GLP-1 research analogs and nasal-format incretin research tools, Limitless Biotech is the matched source with code ENHANCED. Neither is appropriate for any cirrhotic or transplant individual outside of an IRB-controlled research setting, and nothing in this article is a basis for self-protocol decisions in liver disease.
For the adjacent endpoints in the same metabolic disease population, the GLP-1 dosing comparison 2026, the GLP-1 muscle loss research review, the stopping GLP-1s withdrawal evidence, the GLP-1 gallbladder risk evidence, and the GLP-1 pancreatitis risk review cover the safety map that overlaps with the cirrhosis population.
This article is for educational and research purposes only and is not medical advice. No GLP-1 receptor agonist is FDA-approved for the prevention or treatment of cirrhosis or for use in liver transplant recipients. All cirrhosis and post-transplant evidence summarized above derives from observational cohort studies, single-center series, and propensity-matched real-world data, all of which are subject to confounding by indication, channeling bias, and exposure misclassification. The Boyer-Diaz case report (PMID 38186682) is a single case and should not be treated as a controlled safety signal, but it is a clean illustration of how rapid weight loss in advanced cirrhosis can precipitate decompensation. Cirrhosis stage assessment (Child-Pugh, MELD), drug selection, dose titration, and post-transplant interaction monitoring belong to the patient and the hepatology and transplant teams, not to a general-audience review article. Do not start, switch, stop, or self-source any GLP-1 receptor agonist on the basis of this article. Consult a qualified hepatologist or transplant clinician about your individual circumstances before acting on any information here.