At a glance
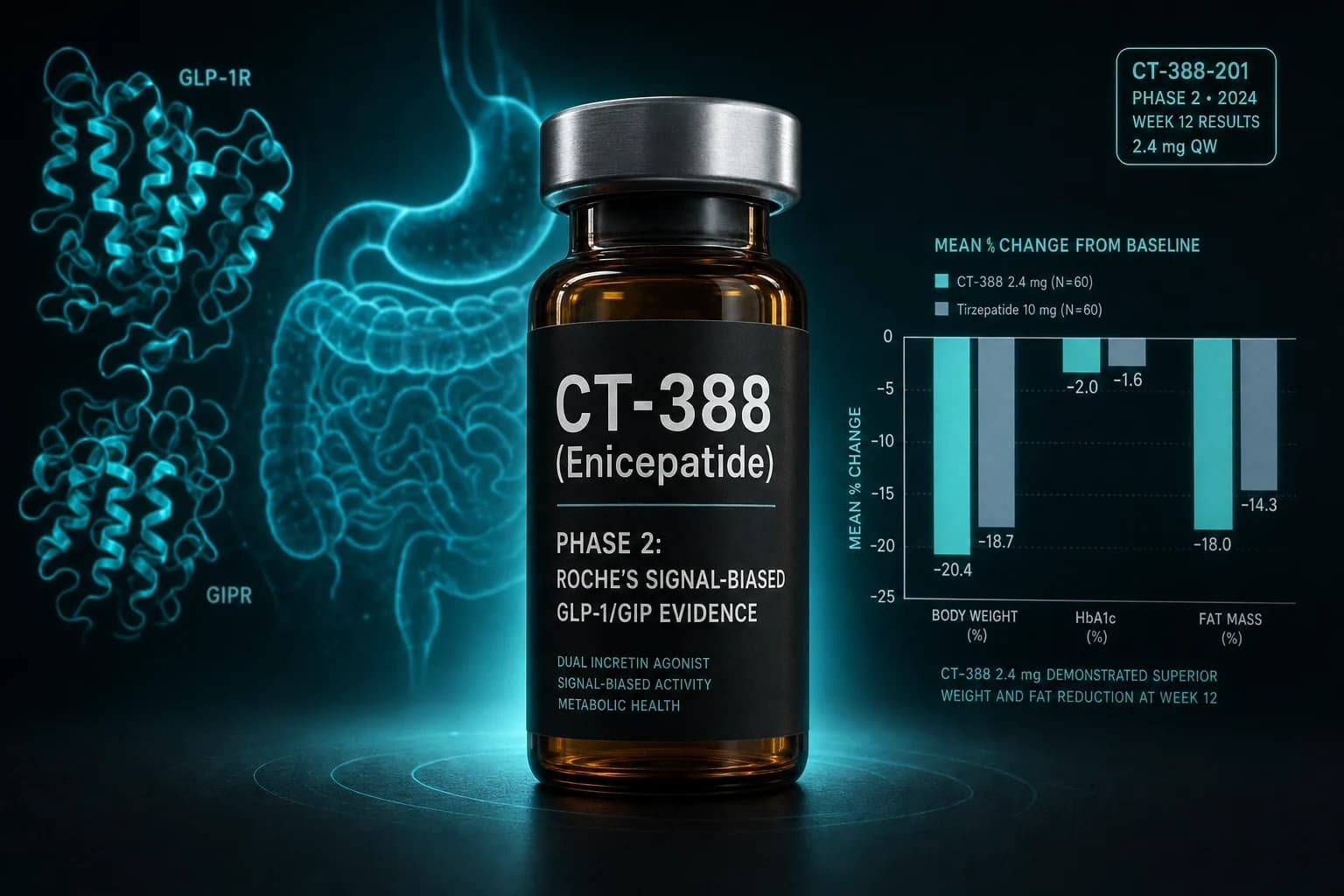
- CT-388 (enicepatide) is Roche's once-weekly subcutaneous GLP-1/GIP dual agonist designed for cAMP signal bias with minimal receptor internalization at both receptors.
- Phase 2 (CT388-103, n=469, 48 weeks): topline 22.5 percent placebo-adjusted weight loss at the 24 mg dose, with no plateau by week 48 (Roche topline, January 27, 2026).
- Phase 1b (n=72, 24 weeks): placebo-adjusted weight loss of 18.8 percent and full normoglycemia in the prediabetic subgroup, published in Cell Metabolism (Chakravarthy et al. 2026, PMID 41319798).
- Discontinuation due to adverse events was 5.9 percent on CT-388 vs 1.3 percent on placebo, with GI events mostly mild to moderate, consistent with the incretin class.
- Phase 3 (Enith-1 and Enith-2) is launching in 2026; no head-to-head trial against tirzepatide or retatrutide is on the public registry yet.
Why CT-388 is the obesity pipeline story Roche needed
For two years, the obesity pipeline conversation was Lilly versus Novo with everyone else in the bleachers. Tirzepatide (Mounjaro / Zepbound) crossed 20 percent average weight loss in SURMOUNT-1. Retatrutide pushed past 24 percent in Phase 2. Roche, late to the category, bought its way in by paying $2.7 billion for Carmot Therapeutics in January 2024 and inheriting CT-388. The bet was that a once-weekly GLP-1/GIP dual agonist designed for a specific receptor signaling profile could close the gap.
On January 27, 2026, Roche announced topline Phase 2 results that, at face value, did exactly that. CT-388 (now carrying the INN enicepatide) hit a placebo-adjusted 22.5 percent body weight reduction at 48 weeks at the high dose, with the curve still falling at the end of the trial. That number matches the tirzepatide 15 mg SURMOUNT-1 result of approximately 20.9 percent placebo-subtracted weight loss at 72 weeks (Jastreboff et al., NEJM 2022, PMID 35658024) on a shorter clock.
Bottom line: CT-388 is a once-weekly signaling-biased GLP-1/GIP dual agonist from Roche/Genentech. Peer-reviewed preclinical and Phase 1b results are published in Cell Metabolism (Chakravarthy et al. 2026). Phase 2 results are sponsor-announced topline. Phase 3 (Enith-1 and Enith-2) starts in 2026. The molecule belongs in the same conversation as tirzepatide, retatrutide, MariTide, and VK2735. It is not yet head-to-head against any of them.
What "signal-biased" actually means at GLP-1R and GIPR
The mechanism is the part most coverage skips. CT-388 is described in the published Cell Metabolism paper as "the first reported clinical-stage unimolecular GLP-1/GIP receptor agonist intentionally designed to activate cAMP signaling with minimal beta-arrestin recruitment at both receptors" (Chakravarthy et al., Cell Metabolism 2026, PMID 41319798). That sentence is doing a lot of work. Three claims sit inside it.
First, cAMP is the canonical second messenger downstream of GLP-1R and GIPR. Sustained cAMP signaling drives insulin secretion in beta cells, satiety signaling in hindbrain neurons, and the rest of the incretin effect. If you keep cAMP up, you keep the metabolic phenotype.
Second, beta-arrestin recruitment is the off switch. When an agonist drives strong beta-arrestin engagement, the receptor is internalized and either recycled or degraded. Lose receptors and you lose the long-tail signal. Native GLP-1 hits this off switch hard, which is part of why endogenous GLP-1 has a half-life under two minutes and why first-generation analogs needed engineering against rapid receptor desensitization.
Third, biasing the agonist toward cAMP and away from beta-arrestin means you can hold the cellular signal longer at lower steady-state doses without losing the receptor itself. Tirzepatide already moved partway in this direction at GLP-1R: prior pharmacology work showed it favors cAMP over beta-arrestin and produces less GLP-1 receptor internalization than native GLP-1 (Willard et al., JCI Insight 2020, DOI 10.1172/jci.insight.140532). Tirzepatide also leans toward the GIP receptor in receptor engagement, which is the imbalanced part of its profile.
CT-388 was engineered to extend that idea further and to both receptors at once. In the published cell-based assays, both GLP-1R and GIPR show minimal receptor internalization compared to native ligands. Whether that pharmacological design translates into a meaningfully different clinical signature than tirzepatide or VK2735 is the open question that the Phase 3 program is built to answer.
Phase 1b: where the peer-reviewed clinical evidence sits
The published clinical dataset is the Phase 1b portion of CT388-101 (NCT04838405). The Cell Metabolism paper reports 72 adults with obesity (BMI at least 30) or overweight with at least one weight-related comorbidity, randomized to once-weekly subcutaneous CT-388 or placebo across multiple ascending dose cohorts, with the longest follow-up cohort treated for 24 weeks at doses titrated up to 22 mg.
Headline efficacy in the Cell Metabolism paper was a placebo-adjusted mean weight loss of 18.8 percent at week 24 (P < 0.001). The dose-response distribution at the high-dose cohort was steep. At week 24, every CT-388-treated participant achieved at least 5 percent weight loss. Eighty-five percent achieved at least 10 percent, 70 percent achieved at least 15 percent, and 45 percent achieved at least 20 percent. The placebo arm produced essentially no mean change, which is the expected pattern in a 24-week obesity Phase 1b without intensive lifestyle co-intervention.
A second signal came out of the glycemic data. In the subgroup of participants with prediabetes at baseline, every CT-388-treated participant returned to normoglycemic ranges by week 24, while the placebo prediabetes group remained largely unchanged. That is a small-N observation, not a powered HbA1c endpoint, but it is consistent with the preclinical glycemic-control data in mice and non-human primates reported in the same Cell Metabolism paper.
For a Phase 1b at 24 weeks, the 18.8 percent placebo-adjusted figure is in the same neighborhood as tirzepatide and ahead of orforglipron at similar time points. The interpretive caveat is that Phase 1b results across small cohorts are notoriously upper-bound. Phase 2 and Phase 3 routinely produce smaller absolute numbers as the cohort widens and adherence pressure realisticizes. The interesting question was always whether the Phase 2 dataset would hold the signal.
Phase 2 (CT388-103): the 22.5 percent topline at 48 weeks
CT388-103 is the randomized, double-blind, placebo-controlled Phase 2 trial in adults with obesity or overweight with at least one weight-related comorbidity. The sponsor-reported design covers 469 participants assigned across low, middle, and high CT-388 dose arms plus placebo, treated for 48 weeks with once-weekly subcutaneous injection and a stepwise titration up to 24 mg. Topline results were announced by Roche and Genentech in a coordinated January 27, 2026 release.
The headline numbers, as reported in the Roche topline announcement and confirmed in the Genentech press release:
| Endpoint at week 48 (CT-388 24 mg vs placebo) | CT-388 24 mg | Placebo | Notes |
|---|---|---|---|
| Placebo-adjusted mean weight loss (efficacy estimand) | 22.5 percent | reference | P < 0.001, no plateau by week 48 |
| Achieved at least 5 percent weight loss | 95.7 percent | not stated | week 48 |
| Achieved at least 10 percent weight loss | 87 percent | not stated | week 48 |
| Achieved at least 20 percent weight loss | 47.8 percent | not stated | week 48 |
| Achieved at least 30 percent weight loss | 26.1 percent | not stated | week 48 |
| Resolution of obesity (BMI under 30) | 54 percent | 13 percent | week 48 |
| Discontinuation due to adverse events | 5.9 percent (across CT-388 arms) | 1.3 percent | full trial |
Three properties of this dataset are worth flagging directly.
First, the 22.5 percent placebo-adjusted figure was generated at 48 weeks, not 72. Tirzepatide's headline SURMOUNT-1 numbers (around 20.9 percent placebo-adjusted at 15 mg) were measured at 72 weeks (Jastreboff et al., NEJM 2022, PMID 35658024). Direct calendar comparison flatters CT-388. A like-for-like 48-week comparison against tirzepatide is not yet published; the SURMOUNT-1 design did not power that interim cut.
Second, the curve was still declining at week 48. The sponsor explicitly noted that the 24 mg dose had not reached a weight-loss plateau by the end of the trial. That is the same pattern reported in the retatrutide Phase 2 trial at 48 weeks (Jastreboff et al., NEJM 2023, PMID 37366315) and is the obesity-pipeline tell that Phase 3 will likely produce a higher peak weight loss number than Phase 2.
Third, the topline is sponsor-announced, not peer-reviewed. Full Phase 2 data, including a per-protocol estimand cut, dose-response by week, glycemic and lipid endpoints, body-composition data, and adverse-event categories, will be presented at an upcoming medical congress and submitted for peer-reviewed publication. Until then, the 22.5 percent number is best treated the way any unpublished topline should be treated: a strong directional read, not a final answer.
How CT-388 sits in the GLP-1 / GIP / glucagon / amylin field
The 2026 obesity-pipeline conversation is no longer about whether GLP-1 receptor agonism works. It is about which receptor combination, at which signaling profile, with which delivery route, against which comparator endpoint. CT-388 belongs in the GLP-1 / GIP dual agonist column. Tirzepatide and VK2735 are the other named entries in that column. Retatrutide adds glucagon. MariTide pairs a GLP-1 agonist with a GIP antagonist, an inverted pharmacology that has its own evidence base in the MariTide writeup. Mazdutide, survodutide, and pemvidutide are GLP-1 / glucagon dual agonists. CagriSema pairs semaglutide with an amylin analog. The pharmacology choices map to different metabolic levers.
| Molecule | Receptor activity | Delivery | Phase reference dataset | Headline weight loss (placebo-adjusted) | Window |
|---|---|---|---|---|---|
| CT-388 (enicepatide) | GLP-1R + GIPR, signal-biased toward cAMP, low internalization | SC weekly | Phase 2 topline (CT388-103, n=469) | ~22.5 percent at 24 mg | 48 weeks |
| Tirzepatide 15 mg | GLP-1R + GIPR, imbalanced toward GIPR | SC weekly | SURMOUNT-1 (n=2539, PMID 35658024) | ~20.9 percent | 72 weeks |
| Retatrutide 12 mg | GLP-1R + GIPR + GCGR (triple) | SC weekly | NEJM Phase 2 (n=338, PMID 37366315) | ~22.1 percent | 48 weeks |
| Semaglutide 2.4 mg | GLP-1R mono | SC weekly | STEP 1 (n=1961, PMID 33567185) | ~12.4 percent | 68 weeks |
| MariTide | GLP-1R agonist + GIPR antagonist | SC monthly | Phase 2 (publicly reported) | ~20 percent at top dose | 52 weeks |
| VK2735 SC | GLP-1R + GIPR (balanced) | SC weekly | Phase 2 VENTURE | ~14.7 percent at 13 weeks (interim) | 13 weeks |
The honest read on this table is that the GLP-1 / GIP / glucagon space is now stacked with molecules that all produce 20-plus percent weight loss in their respective hero datasets. Differentiation in Phase 3 is increasingly going to come from secondary endpoints (lean-mass preservation, cardiometabolic outcomes, real-world tolerability), dose convenience, and price. The pharmacology novelty in CT-388 is the signal-biased design at both receptors. The clinical question is whether that design produces a meaningfully different real-world adherence and adverse-event profile.
Safety and tolerability: what the published and topline data show
The published Phase 1b dataset reported a tolerability profile consistent with the incretin class. Gastrointestinal adverse events (nausea, vomiting, diarrhea, constipation) were the most common, mostly mild to moderate, and concentrated during dose escalation. No new or unexpected safety signals were identified at 24 weeks at doses up to 22 mg.
Phase 2 results preserved that pattern at the longer 48-week window and larger 469-participant cohort. Roche reported that CT-388 was "generally well tolerated" with most gastrointestinal adverse events mild to moderate. The headline tolerability data point is the 5.9 percent treatment-discontinuation rate due to adverse events on CT-388 versus 1.3 percent on placebo. For benchmarking, the SURMOUNT-1 tirzepatide treatment-discontinuation rate due to adverse events was approximately 6 to 7 percent at the highest dose, and the STEP 1 semaglutide rate was approximately 7 percent (Wilding et al., NEJM 2021, PMID 33567185). CT-388 is not obviously worse-tolerated than the GLP-1 standard of care at the headline number, although individual adverse-event category breakdowns are not yet public.
What the topline does not yet show, and what Phase 3 will need to answer: pancreatic enzyme behavior, gallbladder event rates, thyroid C-cell findings if any, injection-site reactions over the long titration, and any signal for cardiovascular events. Those are the cluster the FDA and EMA will care about, and they are the cluster where prior GLP-1 programs have logged label-relevant findings (see the pancreatitis, gallbladder, and thyroid writeups).
Phase 3 (Enith-1 and Enith-2) and the regulatory clock
Roche announced that Phase 3 in obesity (the Enith program, including Enith-1 and Enith-2 as the two pivotal trials) is launching in 2026. The Phase 3 program for CT-388 will need to do three things to support a competitive obesity label. It needs to confirm the Phase 2 weight-loss magnitude at the planned commercial doses across a more diverse trial population. It needs to lock down the cardiovascular and major adverse-event story across long enough follow-up to satisfy regulators. And, increasingly, it needs to produce body-composition and cardiometabolic-outcomes data that compare favorably against the standard of care.
As of June 2026, no head-to-head Phase 3 protocol against tirzepatide has been disclosed publicly. SURMOUNT-5, the published head-to-head of tirzepatide versus semaglutide at SC formulations (Aronne et al., NEJM 2025), set the comparator bar that newer entries will be measured against in real-world prescribing decisions. Whether CT-388 ends up with a SURMOUNT-style head-to-head is one of the most consequential strategic decisions Roche will make in this program.
The parallel Phase 2 program in type 2 diabetes (the "ENICEPATIDE in T2DM" trial registered as a separate study) is the other readout to watch. Tirzepatide entered the market through type 2 diabetes first (SURPASS-2 versus semaglutide 1 mg, Frias et al., NEJM 2021, PMID 34170647) before the obesity indication. CT-388 may follow a similar dual-indication track.
What to actually watch over the next 18 months
Three datapoints will determine whether the 22.5 percent topline holds up as a real differentiator or recedes into the "another 20 percent dual agonist" cluster.
First is the peer-reviewed Phase 2 publication. The full body-composition data, the per-week dose-response curve, the cardiometabolic secondary endpoints, and the per-category adverse-event breakdown all sit there. Until that publication lands, the 22.5 percent number is a strong but unverified directional read.
Second is the Phase 3 obesity readout, expected over the next two to three years. The relevant question is not whether CT-388 produces large weight loss; that is now expected from any dual or triple agonist that reaches Phase 3 in this class. The relevant question is whether the signal-biased pharmacology translates into a measurable advantage on adherence, tolerability, lean-mass preservation, or cardiometabolic outcomes.
Third is whether Roche commits to head-to-head data against tirzepatide or against a triple agonist. Without head-to-head trials, prescribing decisions will collapse to price and availability once a market entry is secured. Roche has the resources and the regulatory experience to run that trial. Whether it does is a strategic decision more than a scientific one.
For researchers and metabolic clinicians tracking the obesity pipeline, the practical takeaway is that CT-388 is a credible Phase 3 entry from a sponsor with the global infrastructure to deliver it. The pharmacology is novel enough to be interesting, the clinical data so far is consistent with the cluster ceiling, and the Phase 3 program is the trial that matters. The next two to three years will tell whether enicepatide becomes the third major branded obesity GLP-1 alongside semaglutide and tirzepatide, or whether it lands in the broader cohort of "approved, similar to the class, modest share" molecules.
Sourcing for researchers tracking the class
Researchers benchmarking new GLP-1 / GIP entries against published reference compounds typically source semaglutide and tirzepatide research vials from vendors that publish lot-level certificates of analysis. Ascension Peptides carries the injectable research compounds in this class, with code ENHANCED for 50 percent off. For oral GLP-1 research analogs and nasal-format incretin research tools, Limitless Biotech is the matched source, with code ENHANCED. CT-388 / enicepatide is a sponsor-controlled investigational molecule and is not sold by research-vial suppliers; bench-pharmacology comparisons rely on published reference compounds plus peer-reviewed CT-388 data, not gray-market enicepatide that does not exist.
For dose-planning across the comparator field, the GLP-1 dosing comparison and the retatrutide vs tirzepatide vs semaglutide writeup cover the published-dose ladders that researchers benchmark against.
This article is for educational and research purposes only and is not medical advice. CT-388 (enicepatide) is an investigational molecule and is not FDA-approved or EMA-approved for any indication as of June 2026. The Phase 2 results discussed above are sponsor-announced topline figures and have not yet been published in a peer-reviewed journal. Phase 1b results are published in Cell Metabolism (Chakravarthy et al. 2026, PMID 41319798). Do not use this article to make decisions about starting, stopping, or sourcing any GLP-1 receptor agonist. Consult a qualified clinician about your individual circumstances before acting on any information here.