At a glance
- KPV is the C-terminal tripeptide (lysine-proline-valine) of α-MSH; retains the anti-inflammatory action without the pigmentary or appetite effects of full-length α-MSH
- Standard oral research dose: 500 mcg once or twice daily, typically encapsulated; PepT1-mediated absorption in the small intestine and inflamed colon
- Mechanism: NF-κB pathway inhibition and IL-1β suppression in enterocytes and epithelial cells (Brzoska et al., 2003)
- Reduced colitis severity in DSS mouse models and inhibited colitis-associated cancer development (Dalmasso et al., 2008; Charrier et al., 2017)
- Compounds well with BPC-157 in research stacks targeting gut mucosal repair plus inflammation control; both peptides act locally in the GI tract
KPV is the smallest piece of α-melanocyte-stimulating hormone that still does the anti-inflammatory work. The tripeptide (lysine-proline-valine, residues 11-13 of α-MSH) retains the cytokine-suppressing and mucosal-protective effects without the appetite-suppression, skin-pigmentation, and central melanocortin signaling of the full 13-amino-acid parent compound. That makes it a clean tool for gut inflammation research: oral dosing, narrow mechanism, low pharmacological cross-talk.
This article covers what KPV actually is at the molecule level, how it gets absorbed, what the published rodent inflammation work shows, the standard research dose protocol, and how it fits with related compounds in IBD-research stacks.
What KPV actually is
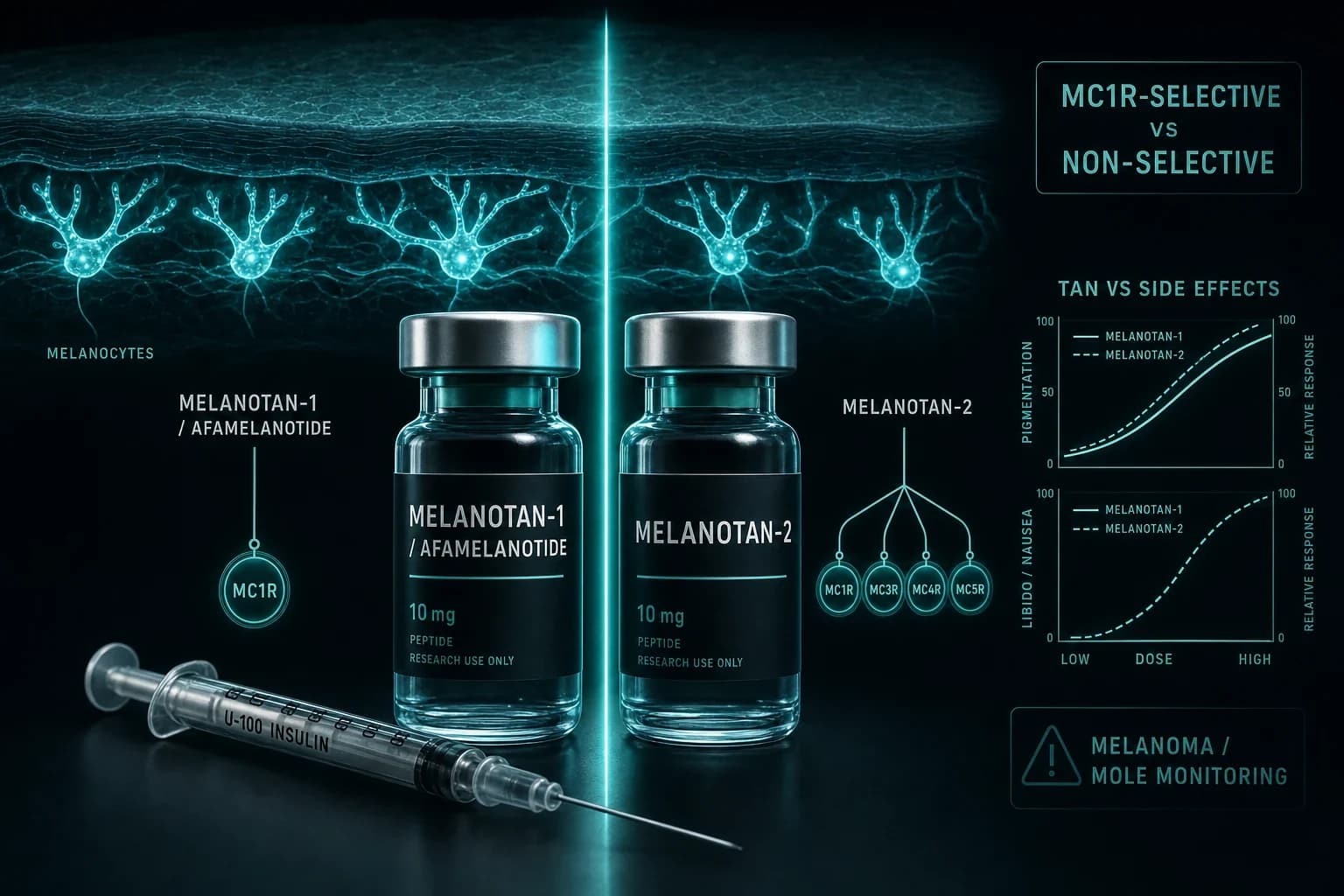
α-MSH is a 13-amino-acid peptide cleaved from proopiomelanocortin (POMC). The full peptide acts on melanocortin receptors (MC1R through MC5R) and drives a range of effects including skin pigmentation, appetite regulation, and anti-inflammatory action. The C-terminal three amino acids (lysine-proline-valine, often written KPV) preserve the anti-inflammatory function but do not engage the melanocortin receptors meaningfully.
This separation is the whole point of KPV as a research compound. The clean anti-inflammatory mechanism without the pigmentary or central effects of full-length α-MSH or Melanotan II is what makes KPV interesting for gut inflammation research, where downstream effects on appetite or skin would be confounding.
The mechanistic dissection was published by Brzoska et al., J Invest Dermatol, 2003, which showed the anti-inflammatory effect of KPV is mechanistically different from the core MSH peptides and likely acts through inhibition of IL-1β signaling rather than through melanocortin receptors.
The PepT1 absorption pathway
For an oral peptide to work at GI inflammation, two things need to be true. First, the compound has to reach the inflamed tissue. Second, it has to enter the cells that are driving the inflammation. KPV does both through a specific transport mechanism.
The human intestinal peptide transporter 1 (hPepT1) is expressed at low levels in the healthy colon but is upregulated during inflammatory bowel disease. KPV is a substrate for PepT1 and is transported into enterocytes by this pathway. Dalmasso et al., Gastroenterology, 2008 demonstrated PepT1-mediated KPV uptake and showed reduced intestinal inflammation in colitis mouse models.
The practical implication: KPV absorption increases at exactly the tissue sites where the inflammation is most active. The drug delivery is naturally targeted because the transporter that brings it in is upregulated by the disease state.
| Property | KPV value |
|---|---|
| Sequence | Lysine-Proline-Valine (Lys-Pro-Val) |
| Molecular weight | ~342 Da |
| Source | C-terminal of α-MSH (residues 11-13) |
| Absorption route | PepT1 transporter, small intestine + inflamed colon |
| Receptor target | None classical; acts via NF-κB / IL-1β inhibition |
| Approved indication | None; research compound |
What the rodent inflammation data shows
The strongest pre-clinical KPV evidence comes from rodent colitis models.
Dextran sulfate sodium (DSS) colitis. DSS-induced colitis is the standard rodent model for ulcerative colitis. Oral KPV reduced colitis severity, body weight loss, and inflammatory cytokine expression in DSS-treated mice (Dalmasso et al., 2008).
Colitis-associated cancer (CAC). Chronic colitis is a risk factor for colorectal cancer. Charrier et al., Mol Cancer, 2017 showed PepT1-mediated KPV reduced tumorigenesis in a murine CAC model using AOM + DSS induction. The mechanism is the same NF-κB and IL-1β inhibition that drives the acute colitis benefit.
Mechanism dissection. Kannengiesser et al., Inflamm Bowel Dis, 2008 characterized the anti-inflammatory activity of KPV in epithelial cells and showed the effect is partially independent of the melanocortin receptors and predominantly mediated through IL-1β pathway inhibition.
Comparison to full α-MSH. Rajora et al., J Leukoc Biol, 1997 showed α-MSH modulates experimental IBD in rodent models, establishing the parent peptide's role. The KPV literature subsequently demonstrated the C-terminal fragment retains the inflammatory benefit while shedding the pigmentary and central effects.
The published evidence is rodent-heavy. Human trials of KPV specifically for IBD have not been published at scale. The mechanism is well-characterized; the human efficacy extrapolation is what most KPV research depends on.
The standard research protocol
Across forum-documented research-use protocols and the rodent-model dose translations, the convergent oral dosing is 500 mcg once or twice daily.
| Phase | Dose | Frequency | Timing | Duration |
|---|---|---|---|---|
| Standard | 500 mcg | Once daily | Morning, fasted or with first meal | 6-12 weeks |
| Higher | 500 mcg | Twice daily | AM and PM | 6-12 weeks |
| Acute inflammation | 1 mg | Once daily | Morning | 4-8 weeks |
Three reasons most protocols use the 500 mcg once-daily dose:
-
PepT1 uptake is saturable. Higher doses do not produce proportionally higher tissue concentrations because the transporter has a maximum throughput. Beyond about 1 mg, additional dose mostly transits unabsorbed.
-
Rodent dose translation supports this range. The mouse colitis studies used doses translating to a human equivalent in the few hundred mcg to 1 mg range using body-surface-area scaling.
-
Tolerance is good across this dose range. Reported side effects are minimal at standard doses. Higher doses do not improve outcomes in published animal work and add no upside.
Most retail oral KPV products ship as capsules at 250-500 mcg per capsule. The compound is reasonably stable at room temperature for the capsule shelf life. Refrigeration is not strictly required but extends shelf life.
Combining KPV with other research peptides
KPV is most commonly stacked with BPC-157 in gut-focused research protocols. The mechanistic logic:
| Peptide | Primary mechanism | Acts where | Best for |
|---|---|---|---|
| KPV | NF-κB / IL-1β inhibition | Inflamed enterocytes (PepT1-mediated) | Gut inflammation, IBD, colitis-adjacent research |
| BPC-157 | Growth factor upregulation, angiogenesis | Local at injury or ulceration site | Mucosal repair, ulcer healing, tissue regeneration |
| Larazotide | Tight junction regulation (zonulin antagonist) | Intestinal barrier | Permeability research |
The pre-mixed KLOW Blend combines KPV with BPC-157, TB-500, and GHK-Cu for gut-plus-recovery research, available from Ascension Peptides with 50% off using code ENHANCED. The oral capsule formulation of KPV combined with BPC-157 and N-Acetyl Larazotide is sold by Limitless Biotech as the Gastro Inflammation Formula with code ENHANCED.
For deeper coverage of KPV in stack context, see the KLOW Blend premium skin + gut recovery protocol. For the broader gut-recovery research framing, see the injectable vs oral peptides bioavailability guide.
Bottom line: KPV's research case is the cleanest small-peptide gut-inflammation intervention with a well-characterized mechanism. The combination with BPC-157 covers both inflammation suppression and mucosal repair through complementary pathways.
Safety and what is known
In rodent studies, KPV has been reported as well tolerated at all doses tested. The most reported observations:
No pigmentary effects. Unlike Melanotan II or the full α-MSH parent, KPV does not engage MC1R meaningfully and does not produce skin pigmentation, melanocyte stimulation, or any sun-tanning effect.
No appetite suppression. Full α-MSH suppresses appetite through MC4R signaling. KPV does not engage MC4R and does not affect food intake or body weight in animal studies.
Minimal GI side effects. The most common reported events in rodent work are mild and transient. Human research-use reports have similarly described tolerable profiles, though the human evidence base is anecdotal.
What the safety database does not cover:
- Long-term human use at therapeutic dosing
- Interactions with immunosuppressive medications
- Use during active autoimmune disease flare versus remission
- Pediatric, pregnancy, and breastfeeding contexts
For researchers running KPV alongside other anti-inflammatory or immunomodulatory compounds, the lack of human interaction data means careful protocol design matters.
How KPV fits the 2026 regulatory landscape
The February 27, 2026 HHS announcement moved 14 of 19 peptides from FDA Category 2 back to Category 1, restoring legal compounding-pharmacy access. KPV was among the peptides included in the reclassification. The practical implication: KPV can now be obtained through licensed compounding pharmacies with a prescription, in addition to the existing research-grade retail channels.
For the broader regulatory context, see the FDA 503A peptide compounding review and the Enhanced Games May 24 article for how the reclassification has reshaped the peptide market this year.
Sourcing
For research-grade oral KPV capsules, Limitless Biotech ships with code ENHANCED. KPV is also part of the Gastro Inflammation Formula (KPV + BPC-157 + N-Acetyl Larazotide) for gut-targeted research. For the injectable KLOW Blend that combines KPV with BPC-157, TB-500, and GHK-Cu, Ascension Peptides ships with 50% off using code ENHANCED.
For our broader sourcing analysis, see the best legit peptide vendors 2026 ranking.
FAQ
What is KPV peptide?
KPV is a tripeptide composed of lysine, proline, and valine (the C-terminal three amino acids of α-melanocyte-stimulating hormone). It retains the anti-inflammatory function of the parent α-MSH peptide without the pigmentary, appetite, or central melanocortin effects. KPV is used in research for gut inflammation, colitis, and IBD-adjacent applications.
What is the standard KPV research dose?
The convergent research-grade protocol is 500 mcg once daily oral, typically in capsule form. Higher doses (twice daily 500 mcg, or 1 mg once daily) are sometimes used in acute inflammation research but do not produce proportionally better outcomes due to PepT1 transporter saturation. Cycle duration is typically 6-12 weeks.
How does KPV work mechanistically?
KPV inhibits NF-κB pathway activation and suppresses IL-1β-mediated inflammatory signaling in epithelial cells and enterocytes. The effect is largely independent of the melanocortin receptors that the parent α-MSH engages. The PepT1 transporter brings KPV into cells, with upregulated PepT1 expression in inflamed tissue creating a naturally targeted delivery mechanism.
Can I take KPV with BPC-157?
Yes, this is one of the most-common research stacks for gut-focused protocols. The two peptides target different mechanisms: KPV inhibits inflammation through NF-κB suppression, while BPC-157 drives mucosal repair through growth factor upregulation and angiogenesis. The pre-mixed KLOW Blend combines them with TB-500 and GHK-Cu; the oral Gastro Inflammation Formula combines KPV with BPC-157 and N-Acetyl Larazotide.
Does KPV cause skin tanning like Melanotan II?
No. KPV does not engage the MC1R receptor that mediates pigmentation. Melanotan II is a synthetic α-MSH analog that strongly activates MC1R and produces tanning. KPV is the C-terminal fragment of α-MSH that retains anti-inflammatory action but does not activate the pigmentary pathway.
Is KPV oral or injectable?
KPV is most commonly used as an oral capsule because the PepT1 transporter pathway makes oral absorption viable, particularly in inflamed tissue where PepT1 is upregulated. Injectable KPV is also available but is less common because the oral route delivers the compound to its primary site of action (intestinal mucosa) more efficiently.
Is KPV legal in the US?
As of the February 27, 2026 HHS reclassification, KPV was moved from FDA Category 2 back to Category 1, restoring legal compounding-pharmacy access. Research-grade KPV is also available through retail peptide vendors with research-use disclosures.
Further reading
- KLOW Blend: premium skin + gut recovery protocol
- Pentadeca arginate (PDA): BPC-157 successor research
- Injectable vs oral peptides: bioavailability guide
- FDA 503A peptide compounding review July 2026
- Best legit peptide vendors 2026
- Thymosin α-1 + BPC-157 combined immune recovery protocol
This article is for educational and research purposes only. KPV is sold under research-use disclosures and is not approved by the FDA for any indication outside of established compounding-pharmacy formulations. None of the content above constitutes medical advice. Consult a qualified clinician for individual medical questions about inflammatory bowel disease or other GI conditions.