At a glance
- Yammine 2021 pilot RCT (n=84): exenatide 2 mg weekly plus a nicotine patch produced 46.3% abstinence vs 26.8% on patch alone at 6 weeks.
- Lengsfeld 2023 RCT (n=255): dulaglutide on top of standard cessation care did not improve 12-week abstinence (63% vs 65%) but blunted post-cessation weight gain by 2.9 kg.
- Hendershot 2026 JAMA Network Open (n=24 non-treatment-seeking smokers): semaglutide cut weekly nicotine craving and weight; cigarettes per day were unchanged vs placebo.
- Wang 2024 Annals of Internal Medicine target-trial emulation (222,942 patients): semaglutide was associated with lower tobacco use disorder healthcare measures vs seven other antidiabetic drug classes.
- Mechanism: GLP-1 receptor activation reduces nicotine reward via nucleus accumbens dopamine and amplifies aversion via the medial habenula to interpeduncular nucleus circuit (Tuesta 2017).
- No GLP-1 RA carries a smoking cessation indication in mid-2026. The strongest practical case is the post-cessation weight gain signal in smokers with overweight or obesity.
In May 2026, JAMA Network Open published the first randomized placebo-controlled trial of semaglutide in adults who smoke daily. The semaglutide arm reported less weekly nicotine craving and a 3.1 kg weight delta versus placebo. Cigarettes per day went down in both arms with no statistically significant separation between them. Twelve people on drug. Twelve on placebo. Nine weeks to a maximum dose of 1.0 mg.
That trial is the most-discussed result in the GLP-1 smoking cessation conversation right now, and it captures the exact problem the field is wrestling with. A real signal on craving and weight. No clean signal on absolute abstinence. No clarity on whether the gap closes at higher doses, in longer follow-up, or in treatment-seeking smokers actively trying to quit.
The honest read on the 2026 evidence is that GLP-1 receptor agonists do something to nicotine reward, the something is consistent across preclinical work and small human trials, and the something has not yet translated into a Phase 3 abstinence advantage over standard cessation care. Varenicline still owns the cessation pharmacology ladder on quit rates. What GLP-1 RAs may eventually own is the comorbid case where a smoker also needs to lose weight, where standard cessation drugs would cause weight gain, and where the metabolic baseline is the dominant clinical concern.
This article walks through what each of the published trials actually showed, what the observational scale data add, what the mechanism story does and does not justify, and where the field sits today.
Bottom line: Three small placebo-controlled RCTs (Yammine 2021 exenatide plus patch n=84, Lengsfeld 2023 dulaglutide n=255, Hendershot 2026 semaglutide n=24) split on abstinence and agree on craving and post-cessation weight. A 222,942-patient observational dataset (Wang 2024, Annals of Internal Medicine) links semaglutide to lower tobacco use disorder healthcare measures. No GLP-1 RA is approved for smoking cessation as of mid-2026.
The headline that built the hype
The single most-cited paper in popular coverage is Wang et al., Ann Intern Med 2024, PMID 39074369. It is a target-trial emulation built on TriNetX electronic health records, which means the authors applied a randomized-trial framework to retrospective EHR data in patients with comorbid type 2 diabetes and tobacco use disorder. The dataset covered 222,942 new starters on antidiabetic medication, of whom 5,967 started semaglutide.
Comparators were the seven other antidiabetic drug classes routinely paired with semaglutide in T2D decision-making (insulins, metformin, DPP-4 inhibitors, SGLT-2 inhibitors, sulfonylureas, thiazolidinediones, and other GLP-1 receptor agonists). The endpoints were practical: medical encounters for tobacco use disorder, smoking cessation counseling visits, and smoking cessation medication prescriptions. Across the seven comparisons, semaglutide initiators had lower rates on every endpoint. The largest separations were against insulins. The smallest, predictably, was against other GLP-1 RAs, which suggests a class effect rather than something molecule-specific to semaglutide.
What the Wang dataset cannot do is establish causality. EHR target-trial emulation controls for measured confounders. It does not control for unmeasured ones, and the prescribing decision for semaglutide in 2018 to 2022 involves unmeasured patient factors that probably correlate with future TUD encounter risk. The authors are explicit about that limit. Their concluding sentence reads that the findings should not be interpreted to justify off-label use for smoking cessation.
The Wang result is best read as the trigger that pulled randomized trial money into this question, not as the answer to it.
The randomized evidence: three trials, three different reads
Three placebo-controlled trials have completed. They use different compounds, different populations, and different endpoints. The signal lines up on craving and weight. It splits on absolute abstinence.
Yammine 2021: exenatide plus nicotine patch increased abstinence in metabolic-risk smokers
Yammine et al., Nicotine Tob Res 2021, PMID 33831213 ran the first GLP-1 smoking cessation pilot RCT. The trial randomized 84 prediabetic or overweight smokers (BMI of at least 27, or HbA1c 5.7 to 6.4%) to extended-release exenatide 2 mg subcutaneously once weekly or placebo for 6 weeks. Both arms received a 21 mg nicotine patch and brief cessation counseling. The primary endpoint was 7-day point-prevalence abstinence at end of treatment, biochemically verified by exhaled CO.
Abstinence was 46.3% on exenatide and 26.8% on placebo. The effect size is large for a 6-week pilot in a smoking trial, where placebo-corrected effect sizes are typically modest. Secondary findings backed the headline: lower end-of-treatment craving in the overall sample, lower withdrawal symptoms among abstainers, and 5.6 lb lower post-cessation body weight on exenatide. Adverse events were higher on exenatide (9.5% vs 2.3%), driven by GI tolerability as expected for the class.
The Yammine trial is small and the population is specific. Both factors limit what can be concluded for general smokers. What it did do was establish that a GLP-1 agonist as add-on to NRT could produce a clean abstinence signal in a metabolic-risk smoker subgroup, which is plausibly the subgroup with the strongest underlying mechanism alignment.
Lengsfeld 2023: dulaglutide did not move abstinence in a larger, general-population trial
Lengsfeld et al., eClinicalMedicine 2023, PMID 36874396 ran the largest completed GLP-1 smoking cessation RCT. The trial randomized 255 adults with moderate-to-severe nicotine dependence at University Hospital Basel to dulaglutide 1.5 mg once weekly or placebo for 12 weeks, all on top of standard varenicline-based cessation care. Abstinence was 63% on dulaglutide and 65% on placebo at end of treatment. That null is the central inconvenient fact in the GLP-1 smoking cessation literature.
Weight told a different story. Post-cessation body weight increased 1.9 kg on placebo and decreased 1.0 kg on dulaglutide, for a baseline-adjusted between-group difference of 2.9 kg in favor of dulaglutide. HbA1c also fell more on dulaglutide. The 12-month follow-up by Lüthi et al., eClinicalMedicine 2024 (doi 10.1016/j.eclinm.2024.102429) reported that the weight benefit faded after the drug was stopped. By 12 months both arms had similar weight trajectories, and abstinence had decayed to roughly 43% vs 41%, with placebo numerically ahead.
Two reads of the Lengsfeld null are competing. One: dulaglutide is a relatively low-potency GLP-1 RA, and the negative result reflects that the molecule does not produce strong enough central activation for an abstinence effect to emerge. Two: GLP-1 RAs as a class do not improve abstinence rates above strong standard care that already includes varenicline, and the apparent abstinence signal in Yammine was specific to NRT-only background care. The 2026 semaglutide trial and the ongoing tirzepatide multi-site trial are designed in part to discriminate between those reads.
Hendershot 2026: semaglutide reduced craving and weight, no abstinence signal in non-treatment-seekers
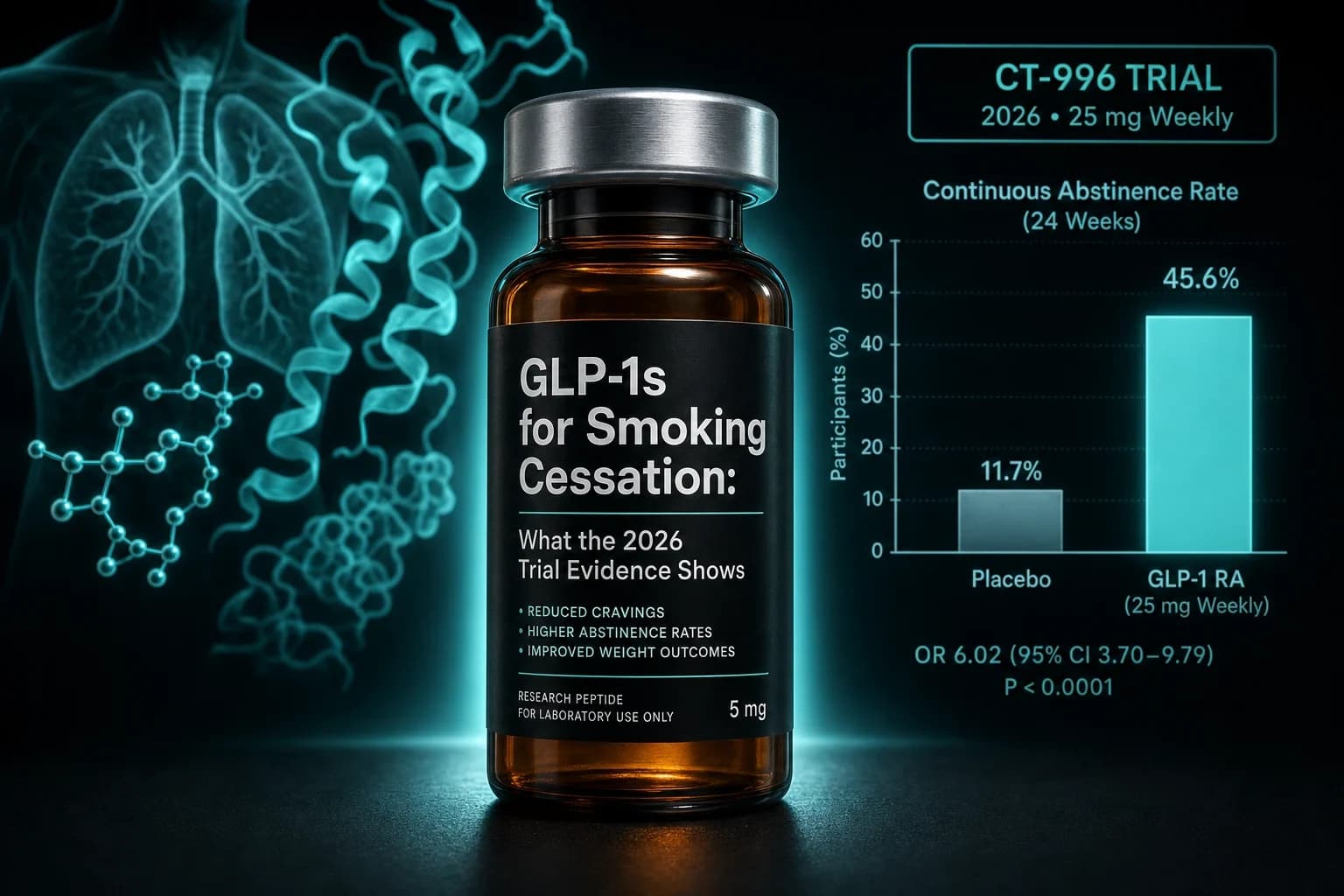
Hendershot et al., JAMA Netw Open 2026 (doi 10.1001/jamanetworkopen.2026.14898) is the most recent placebo-controlled trial and the first formal semaglutide read in cigarette smokers. The trial randomized 24 non-treatment-seeking adults who smoked at least 5 cigarettes per day (mean 15.4 cigarettes per day, mean BMI 33.5, 83% female) to semaglutide titrated from 0.25 to 1.0 mg over 9 weeks, or matched placebo.
Three findings sit at the center of the report. Weekly nicotine craving fell more on semaglutide than on placebo in the preplanned analysis, with a statistically significant separation. Cigarettes per day fell in both arms with no between-group difference. Body weight fell about 3.1 kg more on semaglutide. Adverse events were dominated by GI tolerability consistent with the class.
Three caveats matter. The sample was small (12 per arm) and the trial was single-center. The dose (1.0 mg) sits well below the 2.4 mg weight-management ceiling. The population was not treatment-seeking, which means standard cessation pharmacotherapy expectations do not strictly apply. What the trial captures is the cleanest controlled semaglutide-and-nicotine read available, and the pattern it produced (craving down, smoking similar, weight down) is consistent with the broader literature read that GLP-1 RAs touch nicotine reward without yet showing a Phase 3-grade abstinence signal.
Three trials side by side
| Trial | Compound | Population | Duration / dose | Primary signal | Limit |
|---|---|---|---|---|---|
| Yammine 2021 | Exenatide ER 2 mg/wk + nicotine patch | 84 pre-diabetic or overweight smokers | 6 wk, standard exenatide dose | Abstinence 46.3% vs 26.8% (positive) | Small pilot, specific population |
| Lengsfeld 2023 | Dulaglutide 1.5 mg/wk on top of standard care | 255 nicotine-dependent adults | 12 wk, standard T2D dose | Abstinence null (63% vs 65%); post-cessation weight 2.9 kg lower | No abstinence effect on top of varenicline-based care |
| Hendershot 2026 | Semaglutide 0.25 to 1.0 mg/wk | 24 non-treatment-seeking daily smokers | 9 wk, below weight-management ceiling | Craving down, CPD null, weight 3.1 kg lower | Tiny n, single-center, low dose, non-treatment-seeking |
Bottom line: Abstinence is positive in Yammine, null in Lengsfeld, and not the primary endpoint in Hendershot. Craving and post-cessation weight are positive in every trial that measured them. The class signal lives in the craving and weight axis. The absolute quit-rate axis is unproven.
What the mechanism story does (and does not) carry
GLP-1 receptors are expressed in mesolimbic reward circuits, and the central mechanism in nicotine is now well mapped. Tuesta et al., Nat Neurosci 2017, PMID 28368384 demonstrated that nicotine activates GLP-1 neurons in the nucleus tractus solitarius and that GLP-1 receptor activation in the medial habenula to interpeduncular nucleus aversion pathway abolishes nicotine reward and decreases self-administration in mice. That circuit is the nicotine-specific aversion brake. The Tuesta mechanism is distinct from the classical mesolimbic reward pathway that handles alcohol and cocaine GLP-1 effects.
Earlier preclinical work in Egecioglu et al., PLoS One 2013, PMID 24204788 established that exenatide blunts nicotine-induced locomotor stimulation, accumbal dopamine release, conditioned place preference, and the expression of locomotor sensitization in mice. Together with the Tuesta habenular work, the preclinical evidence base supports a two-circuit model. GLP-1 activation dampens the reward signal from nicotine intake at the mesolimbic dopamine level and amplifies the aversion signal at the medial habenula to interpeduncular nucleus level. On paper, both should reduce drug-seeking.
What the mechanism cannot explain on its own is why the abstinence signal in human trials is so much smaller than the preclinical effect would predict. Two possible explanations are dose and population. Human trials use weight-management or diabetes doses calibrated to peripheral metabolic targets rather than central activation. Most preclinical work uses nicotine-naive animals exposed to short paradigms, while human smokers carry years to decades of receptor adaptation and learned behavior. Both gaps are testable in larger human trials. The multi-site tirzepatide for smoking cessation trial recruiting at USC, Yale, University of Chicago, and University of Colorado Anschutz will produce the first n=300 read on a more potent dual agonist in treatment-seeking smokers.
Why lower craving does not automatically translate into abstinence
A clean way to read the Yammine, Lengsfeld, and Hendershot split is to separate three things smokers experience. The craving impulse. The act of smoking. Sustained abstinence. GLP-1 RAs do something to the first. They do not yet show a clean effect on the third in head-to-head data with standard care.
That gap has two practical interpretations. One is that craving is a necessary but not sufficient mediator of abstinence. Varenicline and bupropion both reduce craving and produce abstinence advantages in Phase 3 trials. A GLP-1 RA that reduces craving without producing the same abstinence advantage is suggesting that the craving-to-abstinence translation depends on factors not captured by GLP-1 activity. The other interpretation is that current trials are underpowered to detect smaller abstinence effects on top of effective standard care, and that the Lengsfeld null is consistent with a real 2 to 3 percentage point effect that simply does not reach significance at n=255.
The pragmatic reader does not need to resolve the question. The trial pipeline will. The relevant question for 2026 to 2028 is whether tirzepatide at chronic weight management doses or semaglutide at 2.4 mg can produce an abstinence advantage on top of varenicline or bupropion. Until that data lands, the realistic 2026 read is craving down, weight down, abstinence unproven.
Where this fits next to the standard cessation ladder
The standard pharmacotherapy ladder for smoking cessation has not moved meaningfully in over a decade. Varenicline remains first-line for most patients with the largest single-drug effect size. Bupropion sits second-line and is useful when depression or weight gain concerns dominate. Nicotine replacement therapy (patch, lozenge, gum) is the floor of any cessation plan and combines well with either of the above. Combination NRT (patch plus short-acting) outperforms single-form NRT in meta-analysis.
| Therapy | Evidence base | Effect on post-cessation weight gain | Where it sits in 2026 |
|---|---|---|---|
| Varenicline | Phase 3, dozens of trials | Modest weight gain similar to NRT | First-line, highest single-drug abstinence effect |
| Bupropion | Phase 3, multiple trials | Slight weight benefit vs placebo | Second-line, useful with comorbid depression |
| Combination NRT | Meta-analysis | Standard cessation weight gain | Floor of any cessation plan |
| Nortriptyline / clonidine | Older RCTs | Variable | Rarely used, tolerability limits |
| Cytisine | Recent Phase 3 | Modest | Approved in Europe and elsewhere, not yet US standard practice |
| GLP-1 RA (off-label) | One positive small RCT, one mid-size null RCT, one small craving-only RCT | 2 to 3 kg weight benefit vs placebo | Off-label, no cessation indication. Weight effect is the strongest case |
What GLP-1 RAs offer that the standard ladder does not is a clean signal on post-cessation weight gain. Smokers gain a mean of 4 to 5 kg in the year after quitting, weight gain is one of the leading causes of cessation failure, and standard cessation pharmacotherapy does not address it. The Lengsfeld and Hendershot data both support a 2 to 3 kg blunting effect during active treatment. For a smoker with metabolic comorbidities, that is a meaningful adjunct on weight grounds independent of any abstinence claim.
Tip: For the smoker with obesity who is starting a GLP-1 RA for weight management and also wants to quit smoking, the existing data supports running both at once with varenicline or NRT as the cessation pharmacotherapy. The GLP-1 RA does the weight work. The cessation drug does the abstinence work. Treat them as additive, not interchangeable.
Who the current evidence actually fits
| Patient profile | Where the 2026 GLP-1 smoking cessation evidence sits |
|---|---|
| Smoker with obesity who also wants to quit | Strongest case for layering a GLP-1 RA onto standard cessation care. Weight benefit is the cleanest finding. |
| Smoker with type 2 diabetes already on insulin or sulfonylureas | Wang dataset shows the largest semaglutide-vs-comparator effect against insulin. A switch to semaglutide is rational on diabetes grounds with a possible smoking-related secondary benefit. |
| Normal-weight smoker with no metabolic indication | Off-label GLP-1 use is not supported by current evidence. The trial evidence is in smokers with overweight, obesity, or dysglycemia. |
| Smoker who failed varenicline | No trial data on this sequence. Theoretically reasonable to consider a GLP-1 RA add-on but unproven. |
| Adolescent smoker | No GLP-1 smoking trial data in adolescents. Pediatric GLP-1 data sits in obesity, not nicotine. See the GLP-1 pediatric obesity evidence breakdown. |
| Pregnancy or planning pregnancy | GLP-1 RAs are contraindicated. NRT remains the preferred cessation aid. |
| Smoker with comorbid alcohol use disorder | Combined AUD-nicotine evidence is preliminary. See the semaglutide alcohol cravings research read for the AUD-specific signal. |
What to track over the next 18 months
Three datasets will move this question.
The multi-site tirzepatide for smoking cessation trial recruiting at USC, Yale, University of Chicago, and University of Colorado Anschutz is the first n=300 read on a more potent dual agonist in treatment-seeking smokers with overweight or obesity. The trial is the closest analog to a Phase 2/3 cessation drug study and is designed to detect a real abstinence advantage if one exists.
A separate semaglutide post-smoking-cessation weight management trial at the University of Texas Health Science Center, Houston, will test the more pragmatic question of whether a GLP-1 RA prevents the weight gain that drives so much cessation failure. That trial uses semaglutide 2.4 mg, the full weight-management dose, and treats abstinence as a coprimary endpoint alongside weight.
Pfizer's commitment to a Phase 3 program for berobenatide includes a knee osteoarthritis arm and an OSA arm but no specific smoking cessation arm at this time. Whether a monthly GLP-1 RA could produce stronger abstinence signals through a smoother pharmacokinetic profile is an interesting question that has not been formally tested. See the berobenatide Pfizer monthly GLP-1 VESPER-3 evidence for the broader berobenatide pipeline.
Outside the GLP-1 class, the cytisine evidence base continues to mature and may move first into the US standard cessation ladder before GLP-1 RAs get there. Cytisine is structurally similar to varenicline, carries comparable Phase 3 evidence, and is meaningfully cheaper. The GLP-1 conversation does not happen in isolation.
What the evidence does not yet show
Five limits worth holding onto before reading any 2026 GLP-1 cessation summary too generously.
First, no Phase 3 trial has reported. The largest controlled trial is 255 participants on dulaglutide with a null abstinence finding. Treat the field as Phase 2 in maturity, not Phase 3.
Second, the observational signal in Wang is consistent with a real effect and is also consistent with prescriber selection. EHR target-trial emulation handles measured confounders. It does not handle unmeasured ones, and which patient gets prescribed semaglutide in 2018 to 2022 carries unmeasured factors that may correlate with future smoking trajectory.
Third, the craving signal is well replicated. The abstinence signal is not. Equating them is the most common error in popular coverage of this class.
Fourth, the post-cessation weight benefit fades after the drug is stopped. The Lüthi 12-month follow-up showed weight convergence by one year in both arms. That is a real-world dosing constraint. A durable weight-only benefit requires continued GLP-1 RA exposure.
Fifth, the safety profile of the GLP-1 RA class still applies. GI tolerability, gallbladder events, theoretical pancreatitis risk, NAION reports in diabetes, and others. The GLP-1 pancreatitis risk evidence review, the GLP-1 gallbladder risk evidence, the GLP-1 NAION vision loss evidence, and the GLP-1 mental health and depression evidence cover the relevant adjacent risks for any smoker considering off-label use.
How the smoking-cessation read compares to the alcohol read
The same lead investigator (Christian Hendershot at USC) has now run placebo-controlled semaglutide trials in both alcohol use disorder and daily cigarette use. The pattern is the same in both: craving moves, the absolute consumption metric moves less, weight moves. The semaglutide alcohol cravings research read goes deeper on the AUD findings, including the larger Wang AUD cohort and the preclinical mechanism work that is shared across substances.
For broader GLP-1 indication context across the class, the semaglutide CKD FLOW evidence, the GLP-1 Alzheimer's EVOKE and ELAD review, and the GLP-1 Parkinson's LIXIPARK and Exenatide-PD3 review cover the parallel GLP-1-for-X-disease programs that share an evidence pattern with nicotine. A strong cardiometabolic baseline. A disease-specific signal that may or may not survive Phase 3.
On dosing context across the class, the GLP-1 dosing comparison 2026 covers titration schedules and tolerability profiles for semaglutide, tirzepatide, retatrutide, and orforglipron. Oral options matter more as cessation pharmacology moves into chronic-use territory, and the orforglipron Phase 3 evidence covers the FDA-approved daily oral small molecule.
Sourcing for researchers
If you are researching GLP-1 receptor agonists in the context of reward circuitry or running protocols outside the standard prescribing channels, the injectable side (semaglutide, tirzepatide, retatrutide) is best sourced through vendors that publish certificates of analysis. Ascension Peptides covers research vials in this class with code ENHANCED for 50% off. Limitless Biotech covers the oral and nasal end with code ENHANCED where those formats apply. Neither replaces a clinician-supervised cessation plan, and tobacco use disorder is not a research-vial protocol. Use these sources for the obesity, longevity, and metabolic research where they belong. Pursue cessation care through primary care or a tobacco treatment specialist.
For reconstitution math, the semaglutide 5mg reconstitution chart and the tirzepatide reconstitution chart cover the common vial sizes, and the reconstitution calculator handles dose-by-volume conversion across compounds.
This article is for educational and research purposes only and is not medical advice. No GLP-1 receptor agonist carries an FDA-approved indication for smoking cessation or tobacco use disorder as of mid-2026, and any use in that context is off-label. The randomized evidence base is small and split. The practical case for layering a GLP-1 RA on top of standard cessation care rests primarily on the post-cessation weight gain reduction signal rather than on an abstinence advantage. Standard first-line cessation pharmacotherapy (varenicline, bupropion, nicotine replacement therapy) and structured behavioral counseling remain the cornerstone of evidence-based tobacco treatment. Consult a primary care clinician or a tobacco treatment specialist before starting, switching, or stopping any therapy.